
Blastomyces dermatitidis — MCQs

A 54-year-old woman comes to the physician because of a painful skin lesion on her right leg for 1 month. It initially started out as a small red spot but has rapidly increased in size during this period. She remembers an ant bite on her leg prior to the lesion occurring. She was treated for anterior uveitis 8 months ago with corticosteroids. She has Crohn's disease, type 2 diabetes mellitus, and hypertension. Current medications include insulin, mesalamine, enalapril, and aspirin. She returned from Wisconsin after visiting her son 2 months ago. Her temperature is 37.6°C (98°F), pulse is 98/min, and blood pressure is 126/88 mm Hg. Examination shows pitting pedal edema of the lower extremities. There is a 4-cm tender ulcerative lesion on the anterior right leg with a central necrotic base and purplish irregular borders. There are dilated tortuous veins in both lower legs. Femoral and pedal pulses are palpated bilaterally. Which of the following is the most likely diagnosis?
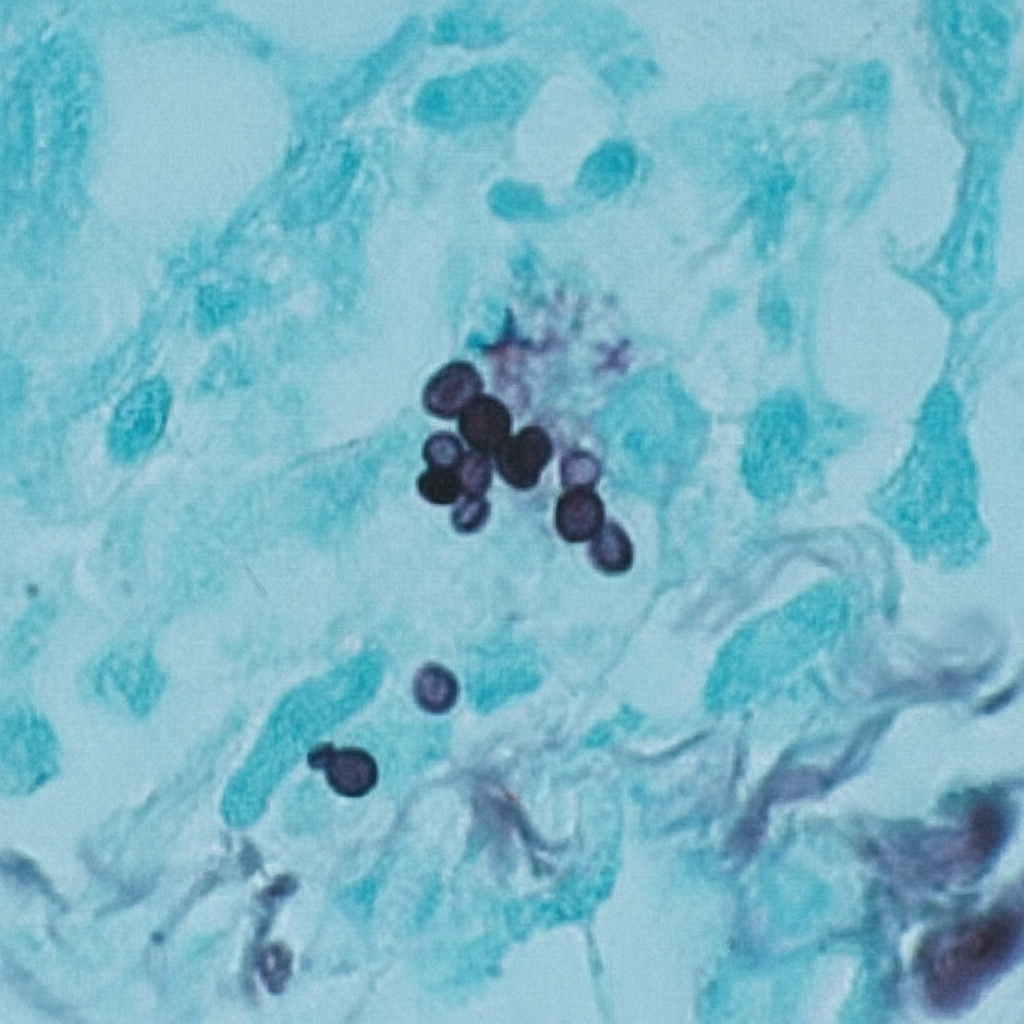
A 44-year-old man comes to the physician because of a 3-week history of productive cough, fever, and lethargy. He also has several skin lesions over his body. His symptoms began 3 weeks after he returned from a camping trip in Kentucky. Three years ago, he underwent kidney transplantation for polycystic kidney disease. Current medications include sirolimus and prednisone. His temperature is 38°C (100.4°F). Diffuse crackles are heard over the lung fields. There are 4 white, verrucous skin patches over his chest and upper limbs. A photomicrograph of a skin biopsy specimen from one of the lesions is shown. Which of the following is the most likely diagnosis?
A young woman from the Ohio River Valley in the United States currently on corticosteroid therapy for ulcerative colitis presented to a clinic complaining of fever, sweat, headache, nonproductive cough, malaise, and general weakness. A chest radiograph revealed patchy pneumonia in the lower lung fields, together with enlarged mediastinal and hilar lymph nodes. Skin changes suggestive of erythema nodosum (i.e. an acute erythematous eruption) were noted. Because the patient was from a region endemic for fungal infections associated with her symptoms and the patient was in close contact with a person presenting similar symptoms, the attending physician suspected that systemic fungal infection might be responsible for this woman’s illness. Which of the following laboratory tests can the physician use to ensure early detection of the disease, and also effectively monitor the treatment response?
An investigator is studying growth patterns of various fungal pathogens. Incubation of an isolated fungus at 25°C shows branching hyphae with rosettes of conidia under light microscopy. After incubation at 37°C, microscopic examination of the same organism instead shows smooth, white colonies with rounded, elongated cells. Infection with the investigated pathogen is most likely to cause which of the following conditions?
A 27-year-old female presents to her primary care physician because she is concerned about lighter colored patches on her skin. She recently went sunbathing and noticed that these areas also did not tan. Her doctor explains that she has a fungal infection of the skin that damages melanocytes by producing acids. She is prescribed selenium sulfide and told to follow-up in one month. Which of the following describes the appearance of the most likely infectious organism under microscopy?
A 40-year-old farmer from Ohio seeks evaluation at a clinic with complaints of a chronic cough, fevers, and anorexia of several months duration. On examination, he has generalized lymphadenopathy with hepatosplenomegaly. A chest radiograph reveals local infiltrates and patchy opacities involving all lung fields. Fine needle aspiration of an enlarged lymph node shows the presence of intracellular yeast. A fungal culture shows the presence of smooth, thin-walled microconidia and tuberculate macroconidia. Which of the following is the most likely diagnosis?
A 4-month-old boy is brought to the physician by his father because of a progressively worsening rash on his buttocks for the last week. He cries during diaper changes and is more fussy than usual. Physical examination of the boy shows erythematous papules and plaques in the bilateral inguinal creases, on the scrotum, and in the gluteal cleft. Small areas of maceration are also present. A diagnosis is made, and treatment with topical clotrimazole is initiated. Microscopic examination of skin scrapings from this patient's rash is most likely to show which of the following findings?
A 3-month-old girl is brought to the emergency department because of a 2-day history of progressive difficulty breathing and a dry cough. Five weeks ago, she was diagnosed with diffuse hemangiomas involving the intrathoracic cavity and started treatment with prednisolone. She appears uncomfortable and in moderate respiratory distress. Her temperature is 38°C (100.4°F), pulse is 150/min, respirations are 50/min, and blood pressure is 88/50 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 87%. Oral examination shows a white plaque covering the tongue that bleeds when scraped. Chest examination shows subcostal and intercostal retractions. Scattered fine crackles and rhonchi are heard throughout both lung fields. Laboratory studies show a leukocyte count of 21,000/mm3 and an increased serum beta-D-glucan concentration. An x-ray of the chest shows symmetrical, diffuse interstitial infiltrates. Which of the following is most likely to confirm the diagnosis?
A 45-year-old HIV-positive patient (CD4 count 180 cells/µL) from San Joaquin Valley presents with erythema nodosum, arthralgias, and bilateral hilar adenopathy. Coccidioides serology shows IgM positive, IgG negative. He is asymptomatic except for joint pain and skin lesions. He is on antiretroviral therapy with undetectable viral load. Evaluate the clinical presentation and synthesize the appropriate management decision considering immune status and disease manifestations.
A 58-year-old man with acute myeloid leukemia presents with breakthrough fungal infection while on fluconazole prophylaxis. Blood cultures grow yeast that forms germ tubes. Chest CT shows new pulmonary nodules. He has neutropenia (ANC 200/µL) and is 2 weeks post-chemotherapy. His serum creatinine is 2.8 mg/dL. Evaluate and synthesize the optimal therapeutic strategy considering drug resistance, organ dysfunction, and underlying malignancy.
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app