
Bacteria — MCQs

On this page
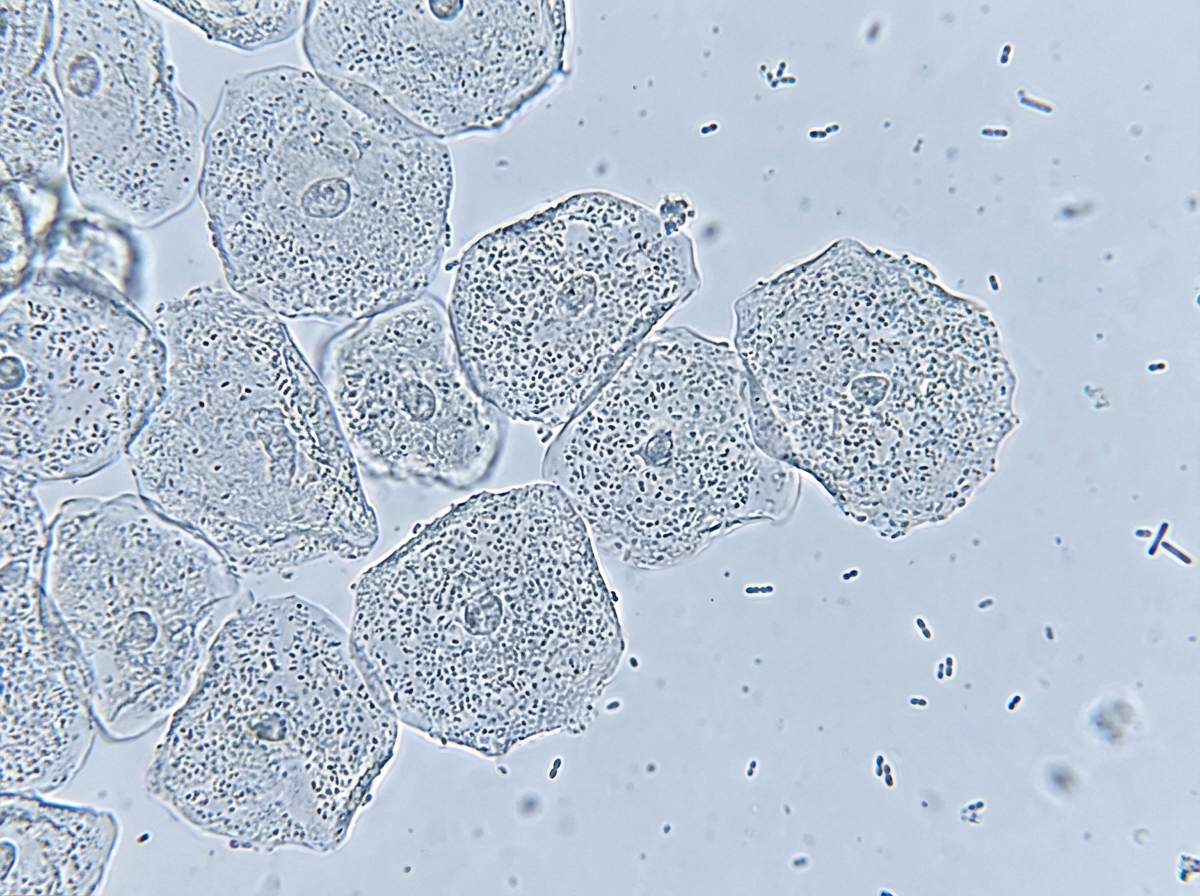
A 25-year-old woman comes to the physician because of vaginal discharge for 4 days. She has no pain or pruritus. Menses occur at regular 27-day intervals and last 5 days. Her last menstrual period was 2 weeks ago. She is sexually active with two male partners and uses a diaphragm for contraception. She had a normal pap smear 3 months ago. She has no history of serious illness and takes no medications. Her temperature is 37.3°C (99°F), pulse is 75/min, and blood pressure is 115/75 mm Hg. Pelvic examination shows a malodorous gray vaginal discharge. The pH of the discharge is 5.0. Microscopic examination of the vaginal discharge is shown. Which of the following is the most likely causal organism?
A 3-year-old female is found to have unusual susceptibility to infections by catalase-producing organisms. This patient likely has a problem with the function of which of the following cell types?
A 28-year-old woman comes to the physician because of a 4-day history of lower abdominal pain and pain with urination. Five months ago, she was treated for gonococcal urethritis. She recently moved in with her newlywed husband. She is sexually active with her husband and they do not use condoms. Her only medication is an oral contraceptive. Her temperature is 37.5°C (99.7°F) and blood pressure is 120/74 mm Hg. There is tenderness to palpation over the pelvic region. Pelvic examination shows a normal-appearing vulva and vagina. Laboratory studies show: Leukocyte count 8,400/mm3 Urine pH 6.7 Protein trace WBC 60/hpf Nitrites positive Bacteria positive Which of the following is the most likely causal organism?
A 12-year-old boy admitted to the intensive care unit 1 day ago for severe pneumonia suddenly develops hypotension. He was started on empiric antibiotics and his blood culture reports are pending. According to the nurse, the patient was doing fine until his blood pressure suddenly dropped. Vital signs include: blood pressure is 88/58 mm Hg, temperature is 39.4°C (103.0°F), pulse is 120/min, and respiratory rate is 24/min. His limbs feel warm. The resident physician decides to start him on intravenous vasopressors, as the blood pressure is not responding to intravenous fluids. The on-call intensivist suspects shock due to a bacterial toxin. What is the primary mechanism responsible for the pathogenesis of this patient's condition?
A 32-year-old man comes to the emergency department because of nausea and vomiting for the past 2 hours. The patient has neither had diarrhea nor fever. Four hours ago he ate some leftover Indian rice dish he had ordered the night before. There is no history of serious illness. He immigrated from India 8 years ago with his family and now works as a butcher. He appears ill. His temperature is 36.7°C (98°F), pulse is 85/min, and blood pressure is 115/70 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 98%. Which of the following is the most likely causal organism?
A researcher is studying the effects of various substances on mature B-cells. She observes that while most substances are only able to promote the production of antibodies when the B-cells are co-cultured with T-cells, a small subset of substances are able to trigger antibody production even in the absence of T-cells. She decides to test these substances that stimulate B-cells alone by injecting them into model organisms. She then analyzes the characteristics of the response that is triggered by these substances. Which of the following correctly describes how the immune response triggered by the B-cell-alone-substances compares with that triggered by substances that also require T-cells?
A 50-year-old male presents to the emergency room complaining of fever, shortness of breath, and diarrhea. He returned from a spa in the Rocky Mountains five days prior. He reports that over the past two days, he developed a fever, cough, dyspnea, and multiple watery stools. His past medical history is notable for major depressive disorder and peptic ulcer disease. He takes omeprazole and paroxetine. He does not smoke and drinks alcohol on social occasions. His temperature is 102.8°F (39.3°C), blood pressure is 120/70 mmHg, pulse is 65/min, and respirations are 20/min. Physical examination reveals dry mucus membranes, delayed capillary refill, and rales at the bilateral lung bases. A basic metabolic panel is shown below: Serum: Na+: 126 mEq/L Cl-: 100 mEq/L K+: 4.1 mEq/L HCO3-: 23 mEq/L Ca2+: 10.1 mg/dL Mg2+: 2.0 mEq/L Urea nitrogen: 14 mg/dL Glucose: 90 mg/dL Creatinine: 1.1 mg/dL Which of the following is the most appropriate growth medium to culture the pathogen responsible for this patient’s condition?
A 26-year-old woman presents to the emergency department with confusion, severe myalgia, fever, and a rash over her inner left thigh. The patient was diagnosed with pharyngitis three days ago and prescribed antibiotics, but she did not take them. Her blood pressure is 90/60 mm Hg, heart rate is 99/min, respiratory rate is 17/min, and temperature is 38.9°C (102.0°F). On physical examination, the patient is disoriented. The posterior wall of her pharynx is erythematous and swollen and protrudes into the pharyngeal lumen. There is a diffuse maculopapular rash over her thighs and abdomen. Which of these surface structures interacts with the causative agent of her condition?
A 32-year-old man with hypertension and gout comes to the physician with left flank pain and bloody urine for two days. He does not smoke cigarettes but drinks two beers daily. Home medications include hydrochlorothiazide and ibuprofen as needed for pain. Physical examination shows left costovertebral angle tenderness. Urine dipstick is strongly positive for blood. Microscopic analysis of a stone found in the urine reveals a composition of magnesium ammonium phosphate. Which of the following is the strongest predisposing factor for this patient's condition?
A 72-year-old patient presents to the emergency department because of abdominal pain, diarrhea, and fever. He was started on levofloxacin for community-acquired pneumonia 2 weeks prior with resolution of his pulmonary symptoms. He has had hypertension for 20 years, for which he takes amlodipine. His temperature is 38.3°C (101.0°F), pulse is 90/min, and blood pressure is 110/70 mm Hg. On examination, mild abdominal distension with minimal tenderness was found. Laboratory tests reveal a peripheral white blood cell count of 12.000/mm3 and a stool guaiac mildly positive for occult blood. Which of the following best describe the mechanism of this patient illness?
Practice by Chapter
Bacterial cell structure and physiology
Practice Questions
Bacterial genetics
Practice Questions
Bacterial metabolism
Practice Questions
Bacterial virulence factors
Practice Questions
Exotoxins and endotoxins
Practice Questions
Bacterial culture methods
Practice Questions
Antimicrobial susceptibility testing
Practice Questions
Bacterial identification methods
Practice Questions
Bacterial taxonomy and classification
Practice Questions
Zoonotic bacterial infections
Practice Questions
Foodborne bacterial pathogens
Practice Questions
Waterborne bacterial pathogens
Practice Questions
Emerging bacterial pathogens
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app