
Bacteria — MCQs

On this page
A 33-year-old woman presents to the urgent care center with 4 days of abdominal pain and increasingly frequent bloody diarrhea. She states that she is currently having 6 episodes of moderate volume diarrhea per day with streaks of blood mixed in. She says she recently returned from a long camping trip with her friends where they cooked all of their own food and drank water from nearby streams. Physical examination is negative for acute tenderness, rebound tenderness, or abnormal bowel sounds. Her vital signs include temperature 38.0°C (100.4°F), blood pressure 106/74 mm Hg, heart rate 94/min, and respiratory rate 14/min. Given the following options, which is the most likely pathogen responsible for her presentation?
A 5-year-old boy presents to the emergency department with a sore throat and trouble breathing. His mother states that his symptoms started last night and have rapidly been worsening. The patient is typically healthy, has received all his childhood immunizations, and currently takes a daily multivitamin. His temperature is 103°F (39.4°C), blood pressure is 100/64 mmHg, pulse is 155/min, respirations are 29/min, and oxygen saturation is 95% on room air. Physical exam is notable for an ill-appearing child who is drooling and is leaning forward to breathe. He does not answer questions and appears very uncomfortable. He will not comply with physical exam to open his mouth for inspection of the oropharynx. Which of the following is the most likely infectious etiology of this patient's symptoms?
An 8-year-old child is brought to the emergency department because of profuse diarrhea and vomiting that have lasted for 2 days. The boy was born at 39 weeks gestation via spontaneous vaginal delivery. He is up to date on all vaccines and is meeting all developmental milestones. Past medical history is noncontributory. The family recently made a trip to India to visit relatives. Today, his heart rate is 100/min, respiratory rate is 22/min, blood pressure is 105/65 mm Hg, and temperature is 37.2ºC (99.0°F). On physical examination, he appears unwell with poor skin turgor and dry oral mucosa. His heart has a regular rate and rhythm and his lungs are clear to auscultation bilaterally. His abdomen is sensitive to shallow and deep palpation. A gross examination of the stool reveals a 'rice water' appearance. Diagnostic microbiology results are pending. Which of the following is the best diagnostic test to aid in the identification of this patient's condition?
Fifteen years ago, a physician was exposed to Mycobacterium tuberculosis during a medical mission trip to Haiti. A current CT scan of his chest reveals respiratory apical granulomas. The formation of this granuloma helped prevent the spread of the infection to other sites. Which pair of cells contributed to the walling-off of this infection?
A 24-year-old woman presents with 3 days of diarrhea. She was recently on vacation in Peru and admits that on her last day of the trip she enjoyed a dinner of the local food and drink. Upon return to the United States the next day, she developed abdominal cramps and watery diarrhea, occurring about 3-5 times per day. She has not noticed any blood or mucous in her stool. Vital signs are stable. On physical examination, she is well appearing in no acute distress. Which of the following is commonly associated with the likely underlying illness?
A 3-year-old boy is brought to the physician for the evaluation of recurrent skin lesions. The episodes of lesions started at the age of 3 months. He has also had several episodes of respiratory tract infections, enlarged lymph nodes, and recurrent fevers since birth. The boy attends daycare. The patient's immunizations are up-to-date. He is at the 5th percentile for length and 10th percentile for weight. He appears ill. Temperature is 38°C (100.4°F). Examination shows several raised, erythematous lesions of different sizes over the face, neck, groin, and extremities; some are purulent. Bilateral cervical and axillary lymphadenopathy are present. What is the most likely underlying mechanism of this patient's symptoms?
A 6-year-old girl is brought to the clinic by her mother with fever, sore throat, and a rash. The patient's mother says that her symptoms started 3 days ago with a high-grade fever, sore throat, vomiting, and malaise. Twenty-four hours later, she says a rash appeared on the patient's neck and, over the next 24 hours, spread to the trunk and extremities. The patient's mother mentions she had a bad sore throat about a week ago but denies any chills, seizures, or sick contacts. The patient has no significant past medical history and takes no current medications. Her birth was uncomplicated, and she has been meeting all developmental milestones. The patient's vital signs include: pulse 90/min, respiratory rate 20/min, temperature 39.0℃ (102.2℉), and blood pressure 90/50 mm Hg. On physical examination, the patient has a whole-body, erythematous punctate, maculopapular rash, as shown in the exhibit (see image). Oropharyngeal examination shows circumoral pallor and a red tongue. The remainder of the examination is unremarkable. Which of the following is the next best step in the management of this patient?

A 23-year-old woman goes to a walk-in clinic while on the fourth day of her honeymoon. She is very upset saying that her honeymoon is being ruined because she is in severe pain. She states that yesterday she began to experience severe pain with urination and seems to be urinating more frequently than normal. She does admit that she has been having increased sexual intercourse with her new husband while on their honeymoon. The physician diagnoses the patient and prescribes trimethoprim-sulfamethoxazole. Which of the following virulence factors is most likely responsible for this patient's infection?
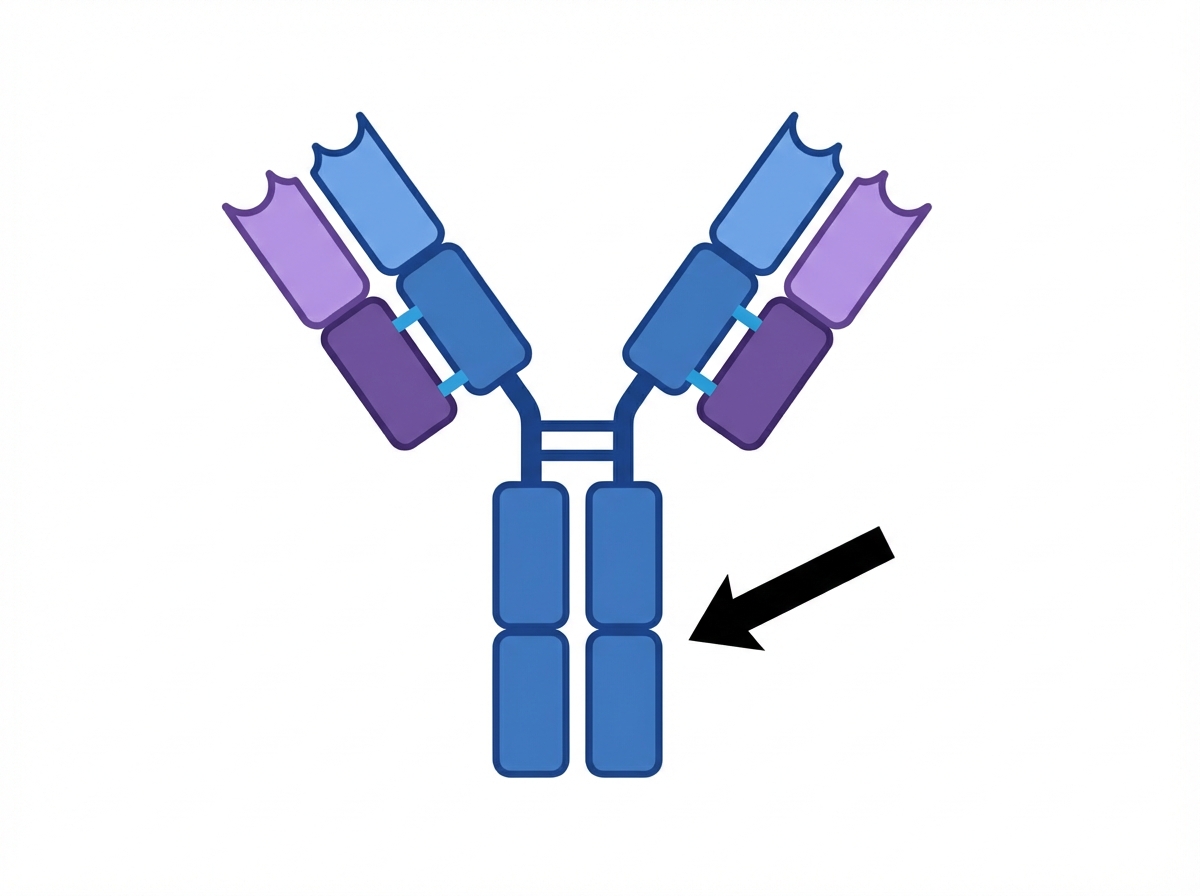
An investigator is studying the structure and function of immunoglobulins that are transmitted across the placenta from mother to fetus. The structure indicated by the arrow is primarily responsible for which of the following immunological events?
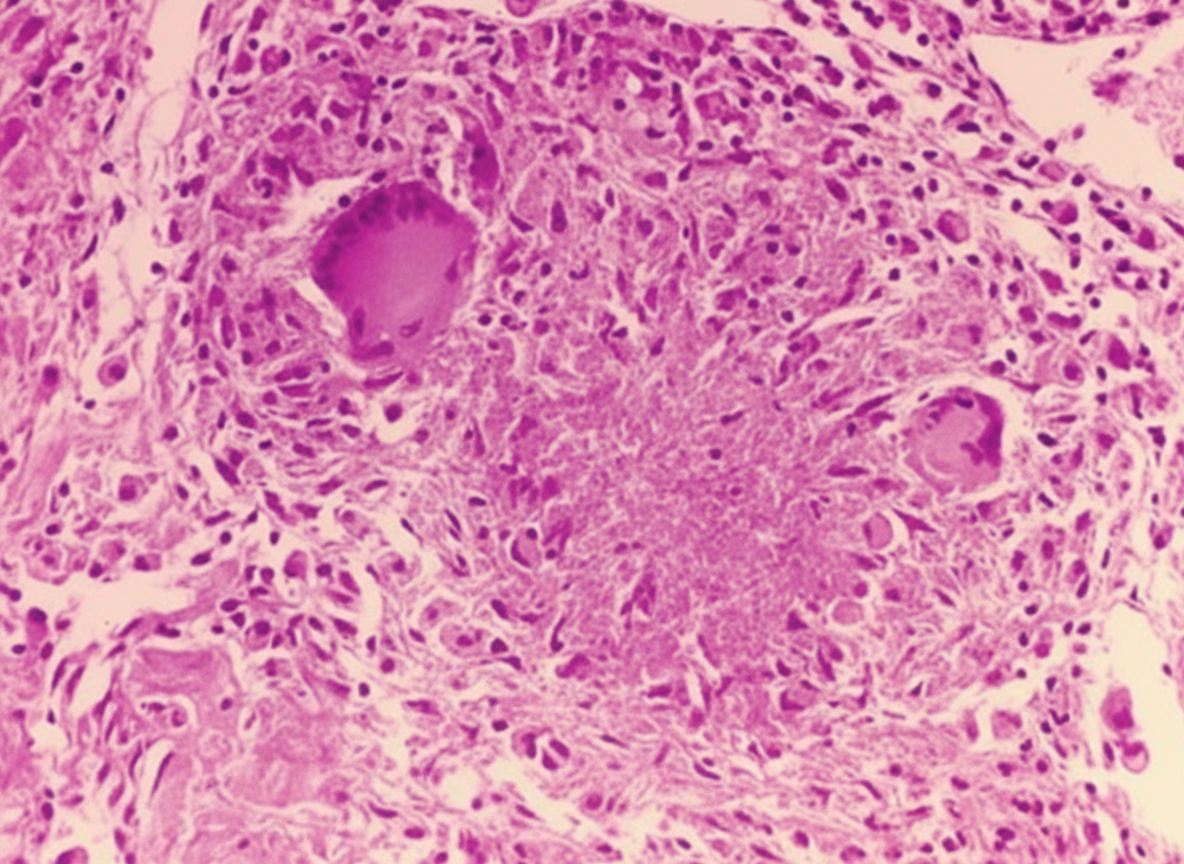
A 48-year-old man who emigrated from Sri Lanka 2 years ago comes to the physician because of a 1-month history of fever, cough, and a 6-kg (13-lb) weight loss. He appears ill. An x-ray of the chest shows patchy infiltrates in the upper lung fields with a cavernous lesion at the right apex. A CT-guided biopsy of the lesion is obtained. A photomicrograph of the biopsy specimen is shown. Which of the following surface antigens is most likely to be found on the cells indicated by the arrow?
Practice by Chapter
Bacterial cell structure and physiology
Practice Questions
Bacterial genetics
Practice Questions
Bacterial metabolism
Practice Questions
Bacterial virulence factors
Practice Questions
Exotoxins and endotoxins
Practice Questions
Bacterial culture methods
Practice Questions
Antimicrobial susceptibility testing
Practice Questions
Bacterial identification methods
Practice Questions
Bacterial taxonomy and classification
Practice Questions
Zoonotic bacterial infections
Practice Questions
Foodborne bacterial pathogens
Practice Questions
Waterborne bacterial pathogens
Practice Questions
Emerging bacterial pathogens
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app