
Bacteria — MCQs

On this page
A 54-year-old woman comes to the physician because of lower back pain, night sweats, and a 5-kg (11-lb) weight loss during the past 4 weeks. She has rheumatoid arthritis treated with adalimumab. Her temperature is 38°C (100.4°F). Physical examination shows tenderness over the T10 and L1 spinous processes. Passive extension of the right hip causes pain in the right lower quadrant. The patient's symptoms are most likely caused by an organism with which of the following virulence factors?
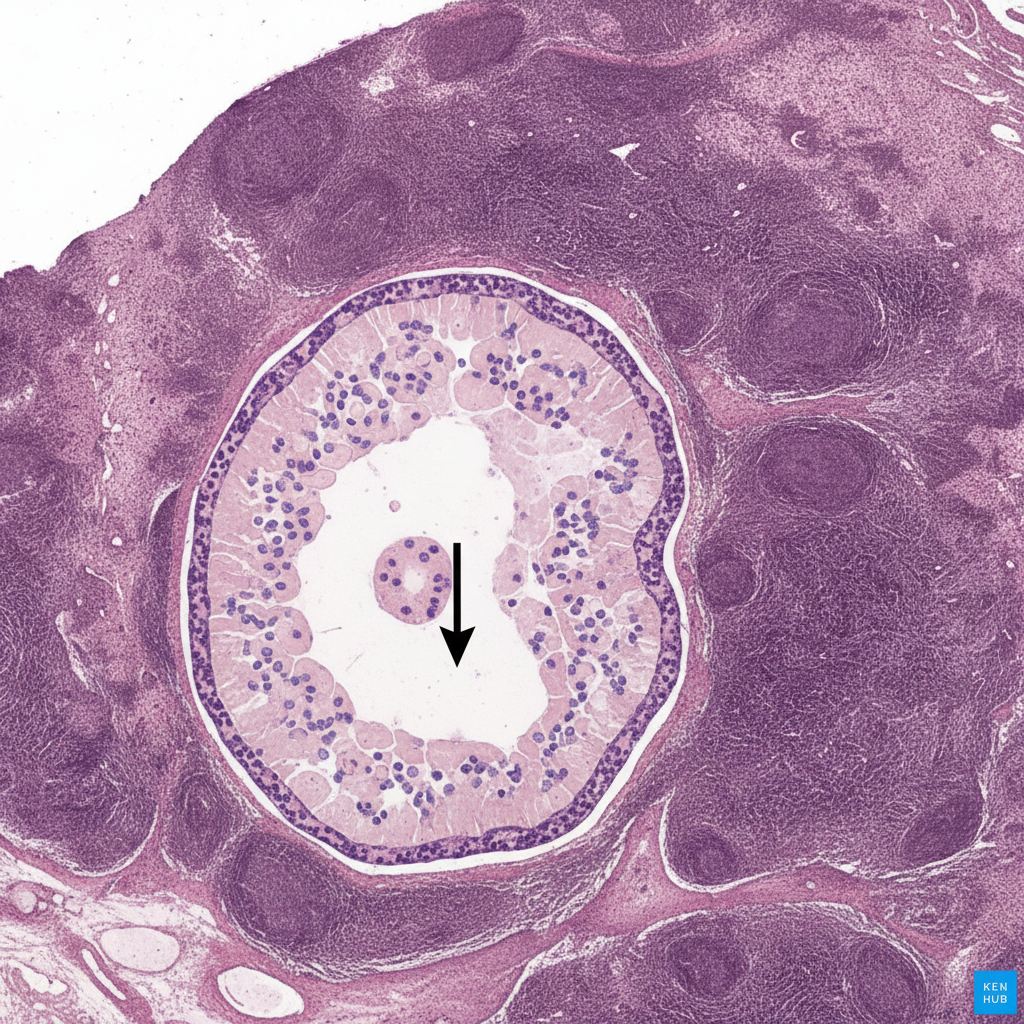
The image shows a cross-section of the appendix with prominent gut-associated lymphoid follicles surrounding the lumen, which is marked by the arrow. Within the germinal centers of these secondary lymphoid follicles, activated B cells receive CD40 signaling from T follicular helper cells and express activation-induced cytidine deaminase (AID). Which immunologic process occurs in these B cells?
A 3-year-old recent immigrant is diagnosed with primary tuberculosis. Her body produces T cells that do not have IL-12 receptors on their surface, and she is noted to have impaired development of Th1 T-helper cells. Which of the following cytokines would benefit this patient?
A 35-year-old patient with no significant past medical history arrives to the ED with abdominal cramps, nausea, and vomiting. He has had no recent travel or chemical exposures; however, three other members of his family also arrived concurrently to the ED with abdominal cramps, nausea, and vomiting. When asked about their recent activities, they recall that they had shared a lunch of leftover fried rice and soft boiled eggs about 5 hours earlier. The patients are otherwise afebrile and deny any history of diarrhea. Which of the following toxins is the most likely to have caused these symptoms?
A 4-year-old male is brought by his mother to the emergency room with dyspnea and fever. His mother reports a two-day history of progressive shortness of breath, malaise, and a fever with a maximum temperature of 101.6°F (38.7°C). The child has visited the emergency room three times over the past two years for pneumonia and otitis media. His family history is notable for sarcoidosis in his mother, diabetes in his father, and an early childhood death in his maternal uncle. His temperature is 101.2°F (38.4°C), blood pressure is 110/90 mmHg, pulse is 110/min, and respirations are 24/min. Physical examination reveals scant lymphoid tissue. A serological analysis reveals decreased levels of IgA, IgG, and IgM. This patient most likely has a defect in a protein that is active in which of the following cellular stages?
An 8-month-old boy is brought to his pediatrician by his parents with a 12-hour history of fever and coughing. He has also been experiencing intermittent diarrhea and skin abscesses since birth. Otherwise, he has been meeting developmental milestones as expected. Analysis of this patient's sputum reveals acute angle branching fungi, and culture shows gram-positive cocci in clusters. A flow cytometry reduction test was obtained that confirmed the diagnosis. Which of the following processes is most likely defective in this patient?
A 32 year-old African American man with a past medical history of sickle cell anemia presents to his primary care physician for a routine check-up. He has no complaints. His physician notes that he likely has an increased susceptibility to infections with certain organisms. Which of the following patient groups has a similar pattern of increased susceptibility?
A 7-year-old boy presents with difficult left eye-opening in the morning, eye discharge, and irritation. These symptoms developed gradually over the past week. He attends a primary school where recently an outbreak of tonsillitis took place. He had otitis media 2 weeks ago treated with ampicillin. At the presentation, the patient’s vital signs are within normal limits. Eye examination reveals bulbar conjunctival injection, mild eyelid edema, and a moderate mucopurulent discharge with crusts on the lower eyelid. There is no corneal or eyelid ulceration. No lymphadenopathy is noted. Which of the following investigations should be performed to establish a diagnosis before the treatment?
A family doctor in a rural area is treating a patient for dyspepsia. The patient had chronic heartburn and abdominal pain for the last 2 months and peptic ulcer disease due to a suspected H. pylori infection. For reasons relating to affordability and accessibility, the doctor decides to perform a diagnostic test in the office that is less invasive and more convenient. Which of the following is the most likely test used?
To protect against a potentially deadly infection, a 19-year-old female receives a vaccine containing capsular polysaccharide. This vaccine will stimulate her immune system to produce antibodies against which organism?
Practice by Chapter
Bacterial cell structure and physiology
Practice Questions
Bacterial genetics
Practice Questions
Bacterial metabolism
Practice Questions
Bacterial virulence factors
Practice Questions
Exotoxins and endotoxins
Practice Questions
Bacterial culture methods
Practice Questions
Antimicrobial susceptibility testing
Practice Questions
Bacterial identification methods
Practice Questions
Bacterial taxonomy and classification
Practice Questions
Zoonotic bacterial infections
Practice Questions
Foodborne bacterial pathogens
Practice Questions
Waterborne bacterial pathogens
Practice Questions
Emerging bacterial pathogens
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app