
Bacteria — MCQs

On this page
An investigator studying immune response administers a 0.5 mL intradermal injection of an autoclaved microorganism to a study volunteer. Four weeks later, there is a 12-mm, indurated, hypopigmented patch over the site of injection. Which of the following is the most likely explanation for the observed skin finding?
A bacterial isolate obtained from a hospitalized patient is found to be resistant to amikacin. The isolated bacteria most likely has which of the following characteristics?
A 32-day-old boy is brought to the emergency department because he is found to be febrile and listless. He was born at home to a G1P1 mother without complications, and his mother has no past medical history. On presentation he is found to be febrile with a bulging tympanic membrane on otoscopic examination. Furthermore, he is found to have an abscess around his rectum that discharges a serosanguinous fluid. Finally, the remnants of the umbilical cord are found to be attached and necrotic. Which of the following processes is most likely abnormal in this patient?
A 32-year-old woman is admitted to the hospital with headache, photophobia, vomiting without nausea, and fever, which have evolved over the last 12 hours. She was diagnosed with systemic lupus erythematosus at 30 years of age and is on immunosuppressive therapy, which includes oral methylprednisolone. She has received vaccinations—meningococcal and pneumococcal vaccination, as well as BCG. Her vital signs are as follows: blood pressure 125/70 mm Hg, heart rate 82/min, respiratory rate 15/min, and temperature 38.7°C (101.7°F). On examination, her GCS score is 15. Pulmonary, cardiac, and abdominal examinations are within normal limits. A neurologic examination does not reveal focal symptoms. Moderate neck stiffness and a positive Brudzinski’s sign are noted. Which of the following would you expect to note in a CSF sample?
A 51-year-old man comes to the physician for 2 months of intermittent low-grade fever, malaise, and joint pain. He has a history of recurrent dental abscesses requiring drainage but has otherwise been healthy. His temperature is 38.3°C (100.9°F) and pulse is 112/min. Physical examination shows a new holosystolic murmur in the left midclavicular line that radiates to the axilla. There are linear reddish-brown lesions underneath the nail beds and tender violaceous nodules on the bilateral thenar eminences. Two sets of blood cultures grow Streptococcus mutans. A transthoracic echocardiogram shows moderate regurgitation of the mitral valve. Which of the following mechanisms is most likely directly involved in the pathogenesis of this patient's valvular condition?
5 days after receiving chemotherapy for ovarian cancer, a 74-year-old woman comes to the physician for a follow-up examination. She feels well and has no complaints. Her leukocyte count is 3,500/mm3 (11% neutrophils and 89% lymphocytes). This patient's profound granulocytopenia is most likely to predispose her to infection with which of the following organisms?
A 43-year-old construction worker presents to the emergency department two hours after sustaining a deep laceration to his left forearm by a piece of soiled and rusted sheet metal. His vital signs are stable, there is no active bleeding, his pain is well controlled, and a hand surgeon has been notified about damage to his forearm tendons. He does not recall receiving any vaccinations in the last 30 years and does not know if he was vaccinated as a child. What is the appropriate post-exposure prophylaxis?
A 22-year-old woman seeks evaluation at a local walk-in clinic for severe lower abdominal pain, vaginal discharge, and painful intercourse for the last couple of weeks. Her last day of menstruation was 1 week ago, and since then the pain has worsened. She is an out-of-town college student engaged in an open relationship with a fellow classmate and another partner from her hometown. Additional concerns include painful micturition and a low-grade fever for the same duration. The physical examination reveals a heart rate of 120/min, respiratory rate of 24/min, and temperature of 38.6°C (101.5°F). The pelvic examination shows an erythematous cervix with a mucopurulent exudate. The cervix bleeds when manipulated with a swab and is extremely tender with movement. Based on the clinical findings, which of the following agents is the most likely cause of her condition?
A 25-year-old woman presents to the ED with a diffuse, erythematous rash in the setting of nausea, vomiting, and fever for 2 days. Physical exam reveals a soaked tampon in her vagina. Blood cultures are negative. The likely cause of this patient's disease binds to which molecule on T cells?
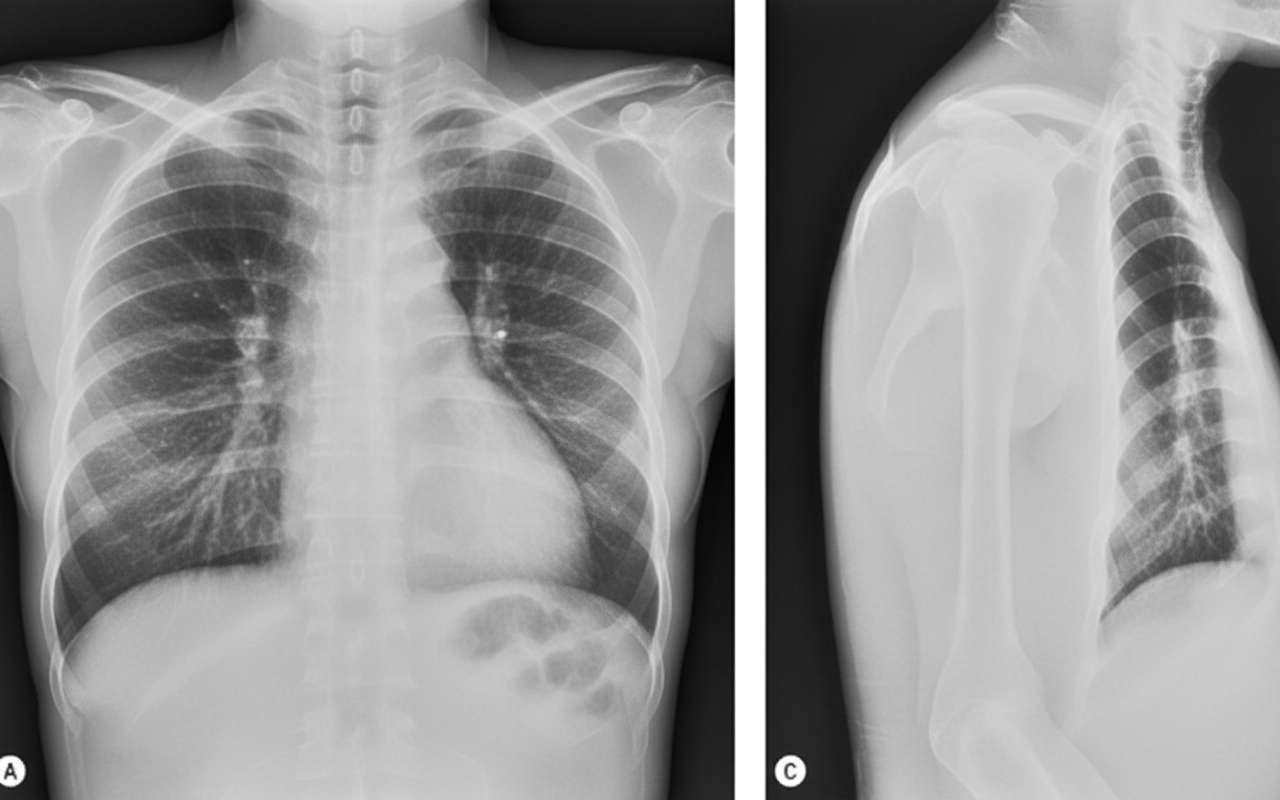
A 65-year-old woman presents to your office after three days of fever and productive cough. She is taking Tylenol for her fever and her last dose was yesterday morning. She reports reddish brown sputum. She has a history of hypertension and hypercholesterolemia for which she takes lisinopril and a statin. She has never smoked and drinks 1-2 glasses of wine a week. She recently returned from Italy and denies having any sick contacts. On physical exam, her temperature is 102.2°F (39°C), blood pressure is 130/78 mmHg, pulse is 90/min, respirations are 21/min, and pulse oximetry is 95% on room air. She has decreased breath sounds in the left lower lobe. Chest x-ray is shown. The causative organism would most likely show which of the following?
Practice by Chapter
Bacterial cell structure and physiology
Practice Questions
Bacterial genetics
Practice Questions
Bacterial metabolism
Practice Questions
Bacterial virulence factors
Practice Questions
Exotoxins and endotoxins
Practice Questions
Bacterial culture methods
Practice Questions
Antimicrobial susceptibility testing
Practice Questions
Bacterial identification methods
Practice Questions
Bacterial taxonomy and classification
Practice Questions
Zoonotic bacterial infections
Practice Questions
Foodborne bacterial pathogens
Practice Questions
Waterborne bacterial pathogens
Practice Questions
Emerging bacterial pathogens
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app