
Bacteria — MCQs

On this page
A 12-year-old boy presents to the emergency room with difficulty breathing after several days of severe sore throat. Further history reveals that his family immigrated recently from Eastern Europe and he has never previously seen a doctor. Physical exam shows cervical lymphadenopathy with extensive neck edema as well as the finding shown in the image provided. You suspect a bacteria that causes the disease by producing an AB type exotoxin. Which of the following is the proper medium to culture the most likely cause of this infection?

A previously healthy 46-year-old woman comes to the physician with a one-week history of productive cough and fatigue. Two weeks ago, she had fever, nasal congestion, rhinorrhea, and myalgias that resolved with supportive care. She has not traveled out of the United States. Pulmonary examination shows dullness to percussion and increased fremitus at the right middle lobe. An x-ray of the chest is shown. A sputum sample is most likely to show which of the following findings?

A scientist is studying the mechanisms by which bacteria become resistant to antibiotics. She begins by obtaining a culture of vancomycin-resistant Enterococcus faecalis and conducts replicate plating experiments. In these experiments, colonies are inoculated onto a membrane and smeared on 2 separate plates, 1 containing vancomycin and the other with no antibiotics. She finds that all of the bacterial colonies are vancomycin resistant because they grow on both plates. She then maintains the bacteria in liquid culture without vancomycin while she performs her other studies. Fifteen generations of bacteria later, she conducts replicate plating experiments again and finds that 20% of the colonies are now sensitive to vancomycin. Which of the following mechanisms is the most likely explanation for why these colonies have become vancomycin sensitive?
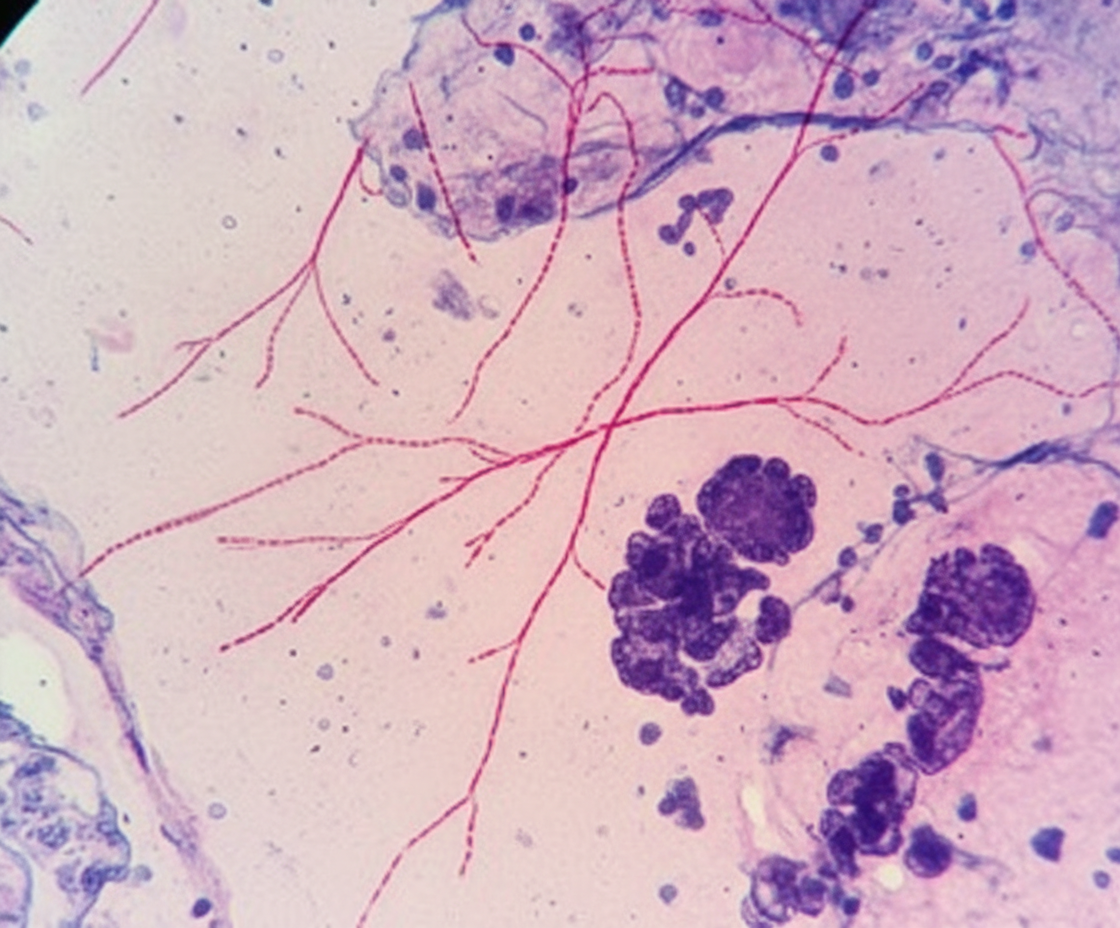
A 68-year-old man comes to the physician because of a 1-month history of fatigue, low-grade fevers, and cough productive of blood-tinged sputum. He has type 2 diabetes mellitus and chronic kidney disease and underwent kidney transplantation 8 months ago. His temperature is 38.9°C (102.1°F) and pulse is 98/min. Examination shows rhonchi in the right lower lung field. An x-ray of the chest shows a right-sided lobar consolidation. A photomicrograph of a specialized acid-fast stained blood-culture isolate is shown. Which of the following is the most likely environmental source of infection for this patient's condition?
A 48-year-old man comes to the physician because of a hypopigmented skin lesion on his finger. He first noticed it 4 weeks ago after cutting his finger with a knife while preparing food. He did not feel the cut. For the past week, he has also had fever, fatigue, and malaise. He has not traveled outside the country since he immigrated from India to join his family in the United States 2 years ago. His temperature is 38.7°C (101.7°F). Physical examination shows a small, healing laceration on the dorsal aspect of the left index finger and an overlying well-defined, hypopigmented macule with raised borders. Sensation to pinprick and light touch is decreased over this area. Which of the following is the most likely causal pathogen of this patient's condition?
An investigator inoculates three different broths with one colony-forming unit of Escherichia coli. Broth A contains 100 μmol of lactose, broth B contains 100 μmol of glucose, and broth C contains both 100 μmol of lactose and 100 μmol of glucose. After 24 hours, the amounts of lactose, galactose, and glucose in the three broths are measured. The results of the experiment are shown: Lactose Galactose Glucose Broth A 43 μmol 11 μmol 9 μmol Broth B 0 μmol 0 μmol 39 μmol Broth C 94 μmol 1 μmol 66 μmol The observed results are most likely due to which of the following properties of broth A compared to broth C?
A 34-year-old, previously healthy woman is admitted to the hospital with abdominal pain and bloody diarrhea. She reports consuming undercooked beef a day before the onset of her symptoms. Her medical history is unremarkable. Vital signs include: blood pressure 100/70 mm Hg, pulse rate 70/min, respiratory rate 16/min, and temperature 36.6℃ (97.9℉). Physical examination shows paleness, face and leg edema, and abdominal tenderness in the lower right quadrant. Laboratory investigation shows the following findings: Erythrocytes 3 x 106/mm3 Hemoglobin 9.4 g/dL Hematocrit 0.45 (45%) Corrected reticulocyte count 5.5% Platelet count 18,000/mm3 Leukocytes 11,750/mm3 Total bilirubin 2.33 mg/dL (39.8 µmol/L) Direct bilirubin 0.2 mg/dL (3.4 µmol/L) Serum creatinine 4.5 mg/dL (397.8 µmol/L) Blood urea nitrogen 35.4 mg/dL (12.6 mmol/L) E. coli O157: H7 was identified in the patient’s stool. Which toxin is likely responsible for her symptoms?
A 20-week-old infant is brought to an urgent care clinic by her mother because she has not been eating well for the past 2 days. The mother said her daughter has also been "floppy" since yesterday morning and has been unable to move or open her eyes since the afternoon of the same day. The child has recently started solid foods, like cereals sweetened with honey. There is no history of loose, watery stools. On examination, the child is lethargic with lax muscle tone. She does not have a fever or apparent respiratory distress. What is the most likely mode of transmission of the pathogen responsible for this patient’s condition?
A 34-year-old man presents with a 2-day history of loose stools, anorexia, malaise, and abdominal pain. He describes the pain as moderate, cramping in character, and diffusely localized to the periumbilical region. His past medical history is unremarkable. He works as a wildlife photographer and, 1 week ago, he was in the Yucatan peninsula capturing the flora and fauna for a magazine. The vital signs include blood pressure 120/60 mm Hg, heart rate 90/min, respiratory rate 18/min, and body temperature 38.0°C (100.4°F). Physical examination is unremarkable. Which of the following is a characteristic of the microorganism most likely responsible for this patient’s symptoms?
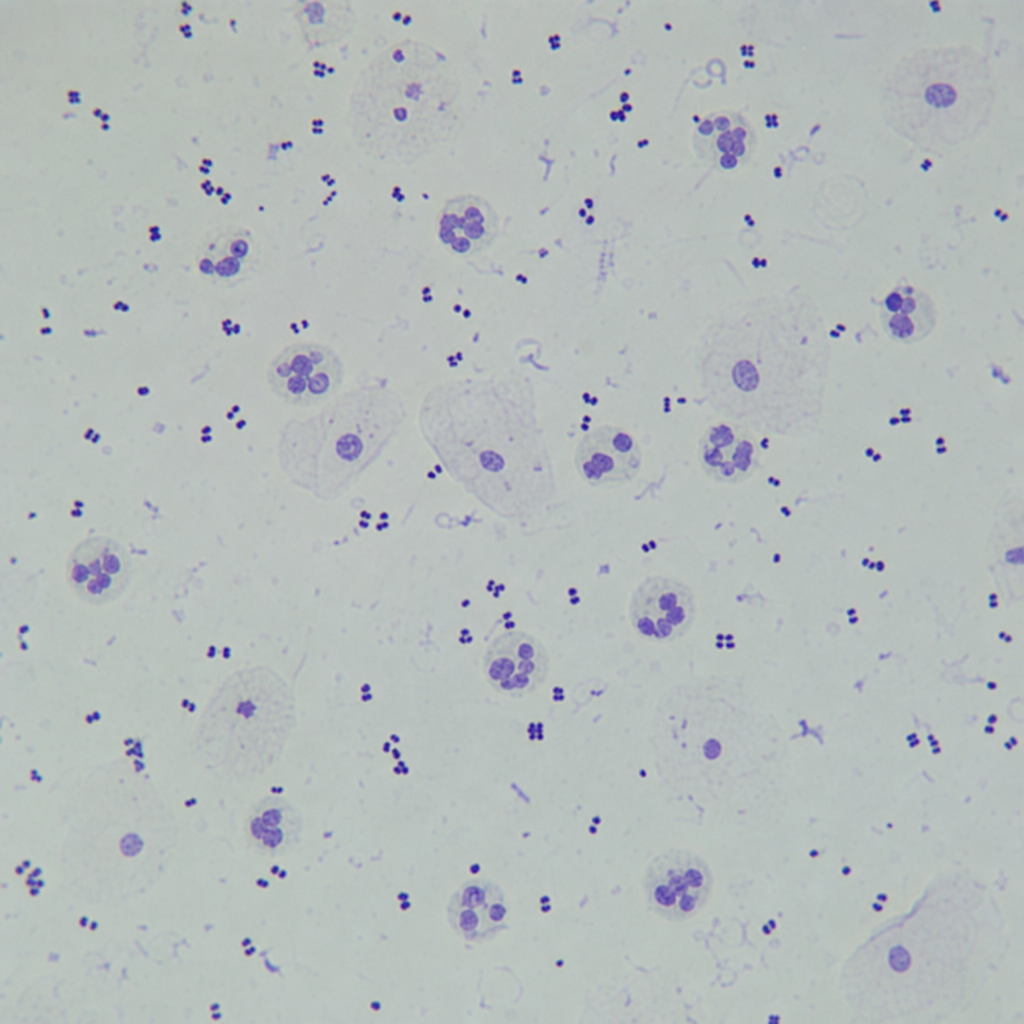
A 25-year-old woman presents to the clinic with complaints of dysuria and increased urinary frequency. Her urinalysis results are negative for nitrites. Urine microscopy shows the findings in figure A. What is the most likely cause underlying her symptoms?
Practice by Chapter
Bacterial cell structure and physiology
Practice Questions
Bacterial genetics
Practice Questions
Bacterial metabolism
Practice Questions
Bacterial virulence factors
Practice Questions
Exotoxins and endotoxins
Practice Questions
Bacterial culture methods
Practice Questions
Antimicrobial susceptibility testing
Practice Questions
Bacterial identification methods
Practice Questions
Bacterial taxonomy and classification
Practice Questions
Zoonotic bacterial infections
Practice Questions
Foodborne bacterial pathogens
Practice Questions
Waterborne bacterial pathogens
Practice Questions
Emerging bacterial pathogens
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app