
Bacteria — MCQs

On this page
A 7-month-old girl is brought to the hospital by her mother, who complains of a lesion on the infant’s labia for the past 5 days. The lesion is 2 x 2 cm in size and red in color with serosanguinous fluid oozing out of the right labia. The parents note that the girl has had a history of recurrent bacterial skin infections with no pus but delayed healing since birth. She also had delayed sloughing of the umbilical cord at birth. Complete blood count results are as follows: Neutrophils on admission Leukocytes 19,000/mm3 Neutrophils 83% Lymphocytes 10% Eosinophils 1% Basophils 1% Monocytes 5% Hemoglobin 14 g/dL Which of the following compounds is most likely to be deficient in this patient?
A 32-year-old woman comes to the emergency department with a 2-day history of abdominal pain and diarrhea. She has had about 8 voluminous stools per day, some of which were bloody. She visited an international food festival three days ago. She takes no medications. Her temperature is 39.5°C (103.1°F), pulse is 90/min, and blood pressure is 110/65 mm Hg. Examination shows a tender abdomen, increased bowel sounds, and dry mucous membranes. Microscopic examination of the stool shows polymorphonuclear leukocytes. Stool culture results are pending. Which of the following most likely caused the patient's symptoms?
A 24-year-old female comes to the physician because of flu-like symptoms and a new rash for 2 days. She denies contacts with sick individuals or recent travel abroad, but recently went camping in Vermont. Vital signs are within normal limits. Examination of the lateral right thigh shows a circular red ring with central clearing. Which of the following is the natural reservoir of the pathogen responsible for this patient's symptoms?
A 13-month-old boy is referred to an immunologist with recurrent otitis media, bacterial sinus infections, and pneumonia, which began several months earlier. He is healthy now, but the recurrent nature of these infections are troubling to his parents and they are hoping to find a definitive cause. The boy was born at 39 weeks gestation via spontaneous vaginal delivery. He is up to date on all vaccines and is meeting all developmental milestones. The patient has five older siblings, but none of them had similar recurrent illnesses. Clinical pathology results suggest very low levels of serum immunoglobulin. As you discuss options for diagnosis with the patient’s family, which of the following tests should be performed next?
A 55-year-old man who recently immigrated to the United States from Azerbaijan comes to the physician because of a 6-week history of recurrent fever, progressive cough with bloody streaks, fatigue, and a 3.6-kg (8-lb) weight loss. He has poorly-controlled type 2 diabetes mellitus treated with insulin. An x-ray of the chest shows a cavitary lesion of the posterior apical segment of the right upper lobe with consolidation of the surrounding parenchyma. He is started on a treatment regimen with a combination of drugs. A culture of the sputum identifies a causal pathogen that is resistant to a drug that alters the metabolism of pyridoxine. Which of the following is the most likely mechanism of resistance to this drug?
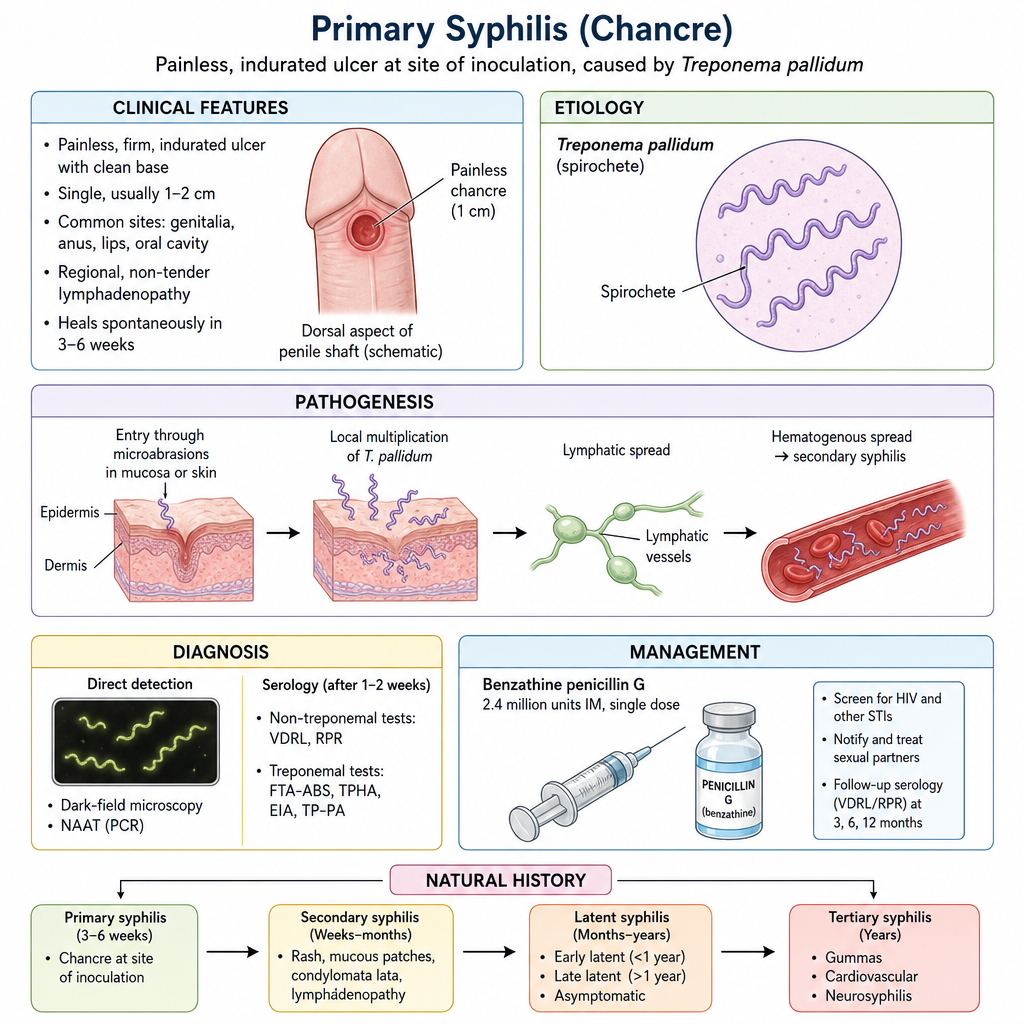
A 25-year-old man presents with an ulcer on his penis. He says that he noticed the ulcer a week ago while taking a shower and it has not improved. He denies any pain, penile discharge, rash, dysuria, fever, or pain on urination. His past medical history is nonsignificant. Sexual history reveals that the patient has had 6 male partners over the past year and uses condoms infrequently. On physical examination, there is a 1-cm ulcer on the dorsal aspect of the penile shaft (see image below). The edge and base of the ulcer are indurated but there is no bleeding or drainage. Two enlarged non-tender inguinal lymph nodes are palpable on the right. There is no evidence of scrotal masses or urethral discharge. A rapid HIV test is negative. Which of the following microorganisms is most likely responsible for this patient’s condition?
A 31-year-old woman presents to the emergency department with a history of fever and vomiting for 2 days and severe headache for a day. Past medical history is significant for migraine diagnosed 10 years ago, but she reports that her current headache is different. She describes the pain as generalized, dull, continuous, severe in intensity, and exacerbated by head movements. Physical examination reveals a blood pressure of 110/76 mm Hg and a temperature of 39.1°C (102.4°F). The patient is awake but in great distress due to pain. A pink-purple petechial rash covers her chest and legs. Extraocular movements are normal. She complains of neck pain and asks you to turn off the lights. Muscle strength is normal in all 4 limbs. Fundoscopic examination is normal. Baseline laboratory investigations are shown: Laboratory test Sodium 145 mEq/L Potassium 3.2 mEq/L Glucose 87 mg/dL Creatinine 1.0 mg/dL White blood cell count 18,900/mm3 Hemoglobin 13.4 g/dL Platelets 165,000/mm3 INR 1.1 Aerobic and anaerobic blood cultures are taken and empiric antibiotics are started. A lumbar puncture is performed. Which of the following cerebrospinal fluid (CSF) findings are expected in this patient?
A 42-year-old man comes to his physician with a history of fever, non-bloody diarrhea, and headache for 10 days. He also complains of anorexia and abdominal pain. He returned from a trip to India 3 weeks ago. His temperature is 40.0°C (104.0°F), pulse is 65/min, respirations are 15/min, and blood pressure is 135/80 mm Hg. He has developed a blanchable rash on his chest and trunk. A photograph of the rash is shown. Examination of the heart, lungs, and abdomen show no abnormalities. Laboratory studies show: Hemoglobin 15 g/dL Mean corpuscular volume 95 μm3 White blood cell count 3400/mm3 Percent segmented neutrophils 40% Which of the following is the most likely diagnosis?

A 4-year-old boy is brought to the clinic by his mother with a history of fever for the past 3 days, yellow nasal discharge, and a severe earache in the right ear. He has no prior history of ear infections and is otherwise healthy. The physician suspects that the infectious agent is Streptococcus pneumoniae and prescribes the appropriate treatment. Which of the following is true about the mechanism of antigen processing in this example?
A 22-year-old woman is brought to the emergency department because of diplopia, slurred speech, progressive upper extremity weakness, and difficulty swallowing for the past several hours. She had mild abdominal pain that resolved spontaneously after returning from her father's farm yesterday. Her temperature is 37°C (98.6°F), respirations are 11/min and labored, and blood pressure is 110/70 mm Hg. Examination shows bilateral nystagmus and ptosis. The pupils are dilated and not reactive to light or accommodation. Muscle strength of the facial muscles and bilateral upper extremities is decreased. Which of the following is the strongest risk factor for this patient's condition?
Practice by Chapter
Bacterial cell structure and physiology
Practice Questions
Bacterial genetics
Practice Questions
Bacterial metabolism
Practice Questions
Bacterial virulence factors
Practice Questions
Exotoxins and endotoxins
Practice Questions
Bacterial culture methods
Practice Questions
Antimicrobial susceptibility testing
Practice Questions
Bacterial identification methods
Practice Questions
Bacterial taxonomy and classification
Practice Questions
Zoonotic bacterial infections
Practice Questions
Foodborne bacterial pathogens
Practice Questions
Waterborne bacterial pathogens
Practice Questions
Emerging bacterial pathogens
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app