
Bacteria — MCQs

On this page
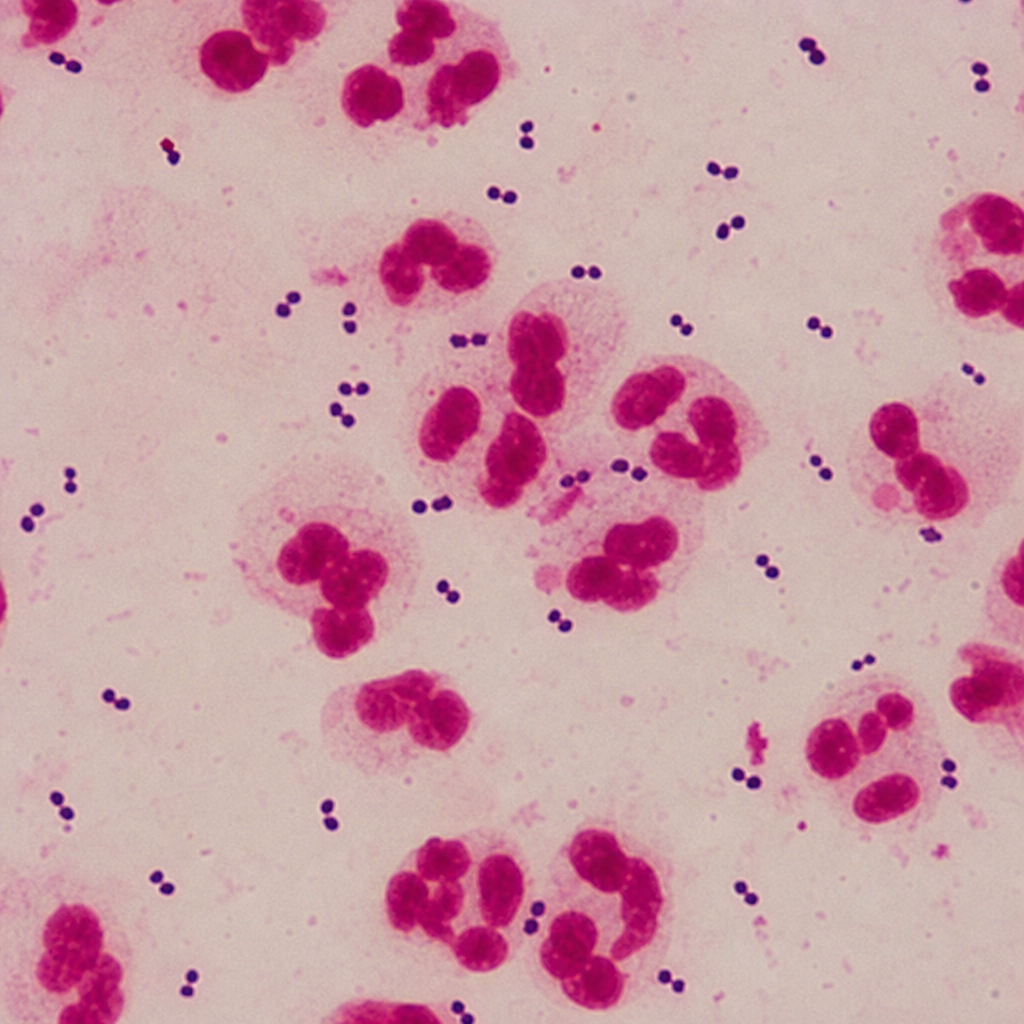
A 19-year-old college student is admitted with fever, nuchal rigidity, and a petechial rash progressing to purpura. Lumbar puncture reveals CSF with WBC 2,800 cells/µL (90% neutrophils), glucose 28 mg/dL (serum glucose 95 mg/dL), and protein 180 mg/dL. A Gram stain of CSF demonstrates Gram-negative diplococci within neutrophils. Blood cultures are pending. The organism is subsequently found to be oxidase-positive and ferments both glucose and maltose. Which of the following characteristics best distinguishes Neisseria meningitidis from Neisseria gonorrhoeae?
A 45-year-old man is brought to the emergency department after being found down outside of a bar. He does not have any identifying information and is difficult to arouse. On presentation, his temperature is 101.2°F (38.4°C), blood pressure is 109/72 mmHg, pulse is 102/min, and respirations are 18/min. Physical exam reveals an ill-appearing and disheveled man with labored breathing and coughing productive of viscous red sputum. Lung auscultation demonstrates consolidation of the left upper lobe of the patient. Given these findings, cultures are obtained and broad spectrum antibiotics are administered. Which of the following agar types should be used to culture the most likely organism in this case?
A 9-year-old girl comes to the clinic with a chief complaint of a swollen eye and sinus infection for 4 days. She complained of left nasal pain prior to these symptoms. The patient noticed that the swelling and redness of her left eye has progressively worsened. It has been difficult to open her eyelids, and she complains of diplopia and pain during ocular movement. The visual acuity is 20/20 in both eyes. Intraocular pressure measurement shows values of 23 and 14 mm Hg in the right and left eyes, respectively. The test results for the complete blood count, ESR, and CRP are as follows (on admission): CBC results Leukocytes 18,000 cells/mm3 Neutrophils 80% Lymphocytes 14% Eosinophils 1% Basophils 0% Monocytes 5% Hemoglobin 12 g/dL ESR 65 CRP 4.6 The organism causing the above condition is destroyed by which one of the following immunological processes?
A 40-year-old man presents to a community health center for a routine check-up. The medical history is significant for a major depressive disorder that began around the time he arrived in the United States from India, his native country. For the last few months, he has been living in the local homeless shelter and also reports being incarcerated for an extended period of time. The patient has smoked 1 pack of cigarettes daily for the last 20 years. The vital signs include the following: the heart rate is 68/min, the respiratory rate is 18/min, the temperature is 37.1°C (98.8°F), and the blood pressure is 130/88 mm Hg. He appears unkempt and speaks in a monotone. Coarse breath sounds are auscultated in the lung bases bilaterally. Which of the following is recommended for this patient?
A 28-year-old man presents to the office complaining of a sore throat, difficulty swallowing, and difficulty opening his mouth for the past 5 days. He states that he had symptoms like this before and "was given some antibiotics that made him feel better". He is up to date on his immunizations. On examination, his temperature is 39.5°C (103.2°F) and he has bilateral cervical lymphadenopathy. An oropharyngeal exam is difficult, because the patient finds it painful to fully open his mouth. However, you are able to view an erythematous pharynx as well as a large, unilateral lesion superior to the left tonsil. A rapid antigen detection test is negative. Based on this clinical presentation, what is a serious complication of the most likely diagnosis?
Which of the following events is likely to occur in the germinal center?
A previously healthy 24-year-old woman comes to the physician because of a 1-day history of nausea and weakness. She is sexually active with 2 male partners and uses an oral contraceptive; she uses condoms inconsistently. Her last menstrual period was 4 days ago. Her temperature is 38.4°C (101°F). Physical examination shows right costovertebral angle tenderness. Pelvic examination is normal. Which of the following is the most likely cause of this patient's condition?
A 2-day-old boy born to a primigravida with no complications has an ear infection. He is treated with antibiotics and sent home. His parents bring him back 1 month later with an erythematous and swollen umbilical cord still attached to the umbilicus. A complete blood cell count shows the following: Hemoglobin 18.1 g/dL Hematocrit 43.7% Leukocyte count 13,000/mm3 Neutrophils 85% Lymphocytes 10% Monocytes 5% Platelet count 170,000/mm3 The immunoglobulin levels are normal. The absence or deficiency of which of the following most likely led to this patient’s condition?
An 18-year-old college freshman scrapes his knee after falling from his bike. He applies some topical neomycin because he knows that it has antibiotic properties. As he is also in biology class, he decides to research the mechanism of action of neomycin and finds that it interferes with formation of the 30S initiation complex in bacteria. What is the messenger RNA (mRNA) signal recognized by the 30S ribosomal subunit necessary for the initiation of translation?
A 55-year-old man with type 2 diabetes mellitus comes to the physician because of a 4-day history of fever, chills, nausea, and abdominal pain. He does not use illicit drugs. His temperature is 39°C (102.2°F). Physical examination shows right upper quadrant tenderness. Ultrasonography of the abdomen shows a 6-cm solitary, fluid-filled cavity in the right hepatic lobe. CT-guided percutaneous aspiration of the cavity produces yellowish-green fluid. Culture of the aspirated fluid grows gram-negative, lactose-fermenting rods. Which of the following is the most likely cause of the color of the aspirated fluid?
Practice by Chapter
Bacterial cell structure and physiology
Practice Questions
Bacterial genetics
Practice Questions
Bacterial metabolism
Practice Questions
Bacterial virulence factors
Practice Questions
Exotoxins and endotoxins
Practice Questions
Bacterial culture methods
Practice Questions
Antimicrobial susceptibility testing
Practice Questions
Bacterial identification methods
Practice Questions
Bacterial taxonomy and classification
Practice Questions
Zoonotic bacterial infections
Practice Questions
Foodborne bacterial pathogens
Practice Questions
Waterborne bacterial pathogens
Practice Questions
Emerging bacterial pathogens
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app