
Atypical — MCQs

On this page
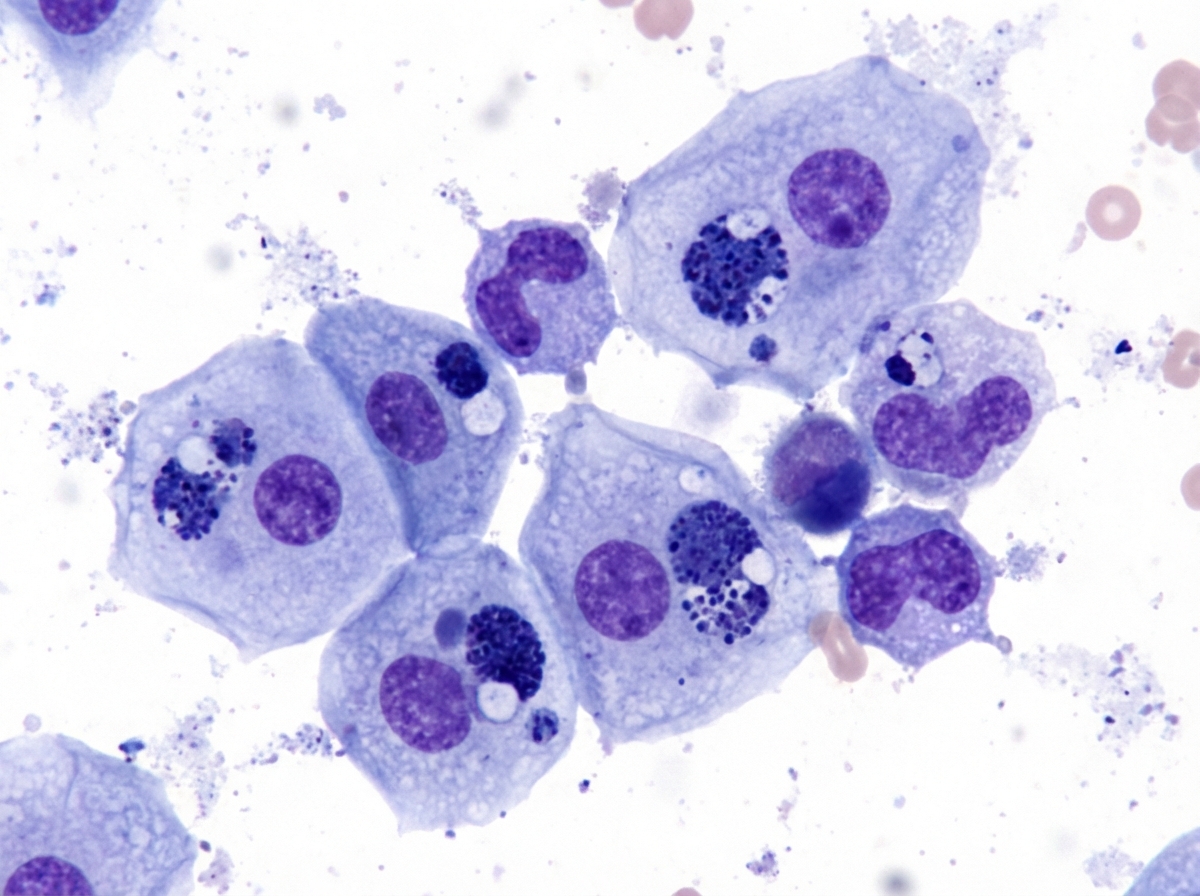
A sample is taken of an ulcer in the inguinal region of a 29-year-old Malaysian male who has had unprotected sex in the past few months. Intracytoplasmic inclusions are seen in the Giemsa staining in Image A. On which of the following can the organism in the staining be grown?
A 22-year-old woman presents to her primary care provider with an unrelenting headache accompanied by fever, chills, and malaise for the past 4 days. She also complains of an earache and dry hacking cough. Past medical history is noncontributory. She takes oral contraceptives and a multivitamin with calcium daily. She drinks alcohol socially and smokes occasionally. Today, her temperature is 37.9°C (100.2°F), pulse is 104/min, respiratory rate is 20/min and blood pressure is 102/82 mm Hg. On physical exam, she appears uncomfortable, but not ill. Her heart rate is elevated with a regular rhythm and her lungs have mild rhonchi in the lower lobes bilaterally. A chest X-ray shows patchy, diffuse infiltrates of the interstitium bilaterally that is worse in the lower lobes. A sputum culture is taken for stereomicroscopy. The pathogen organism appears small, pleomorphic, and lacks a cell wall. Which of the following is the most likely pathogen?
A 32-year-old man comes to the physician because of low-grade fever, dry cough, and shortness of breath. His symptoms began 6 days ago while he was on vacation in Thailand where he went to an urgent care clinic and was started on cefuroxime. His temperature is 38.2°C (100.8°F). Physical examination shows decreased breath sounds at bilateral lung bases. An x-ray of the chest shows diffuse patchy infiltrates. Sputum analysis shows numerous neutrophils but no organisms. Giemsa stain shows epithelial cells with cytoplasmic inclusion bodies. This patient's condition did not improve after the initial treatment because of which of the following properties of the most likely causal pathogen?
A previously healthy 24-year-old woman comes to the physician because of fever, headache, myalgia, photophobia, and a nonproductive cough for 2 days. Three weeks ago, she received a parrot as a birthday present. Her temperature is 38.5°C (101.3°F). Pulmonary examination shows crackles at both lung bases. Her leukocyte count is 8,000/mm3. An x-ray of the chest shows diffuse patchy infiltrates that are most prominent in the lower lobes. Which of the following is the most likely causal organism?
A 45-year-old man presents to the physician with a complaint of recurrent chest pain for the last 2 weeks. He mentions that the pain is not present at rest, but when he walks for some distance, he feels pain like a pressure over the retrosternal region. The pain disappears within a few minutes of stopping the physical activity. He is an otherwise healthy man with no known medical disorder. He does not smoke or have any known dependence. There is no family history of ischemic heart disease or vascular disorder. On physical examination, his vital signs, including blood pressure, are normal. The diagnosis of coronary artery disease due to atherosclerosis is made. Which of the following is known to be an infection associated with this patient’s condition?
A 32-year-old man comes to the physician because of severe burning with urination for the past 3 days. During this period, he has had clear urethral discharge early in the morning. He has no history of serious illness, except for a rash following treatment with erythromycin 20 years ago. The patient takes no medications. He is sexually active with one male and one female partner; they use condoms inconsistently. His younger brother was diagnosed with Crohn disease at the age of 24 years. The patient does not smoke. He drinks one to two beers on weekends. He appears well. Temperature is 36.8°C (98°F), pulse is 75/min, and blood pressure is 135/78 mm Hg. Physical examination shows no abnormalities. Gram stain of a urethral swab shows neutrophils but no organisms. Which of the following is the most likely causal pathogen?
A previously healthy 25-year-old man comes to the physician because of a 1-week history of fever and fluid release from painful lumps in his right groin. He had an atraumatic ulceration of his penis about 1 month ago that was not painful and resolved on its own within 1 week. He works at an animal shelter for abandoned pets. He is sexually active with multiple male partners and does not use condoms. His temperature is 38.5°C (101.3°F). Examination of the groin shows numerous tender nodules with purulent discharge. The remainder of the examination shows no abnormalities. Which of the following is the most likely causal pathogen?
Practice by Chapter
Mycoplasma pneumoniae
Practice Questions
Chlamydia pneumoniae
Practice Questions
Chlamydia trachomatis
Practice Questions
Chlamydia psittaci
Practice Questions
Rickettsia species
Practice Questions
Coxiella burnetii
Practice Questions
Ehrlichia and Anaplasma
Practice Questions
Spirochetes overview
Practice Questions
Treponema pallidum
Practice Questions
Borrelia species
Practice Questions
Leptospira species
Practice Questions
Mycobacteria overview
Practice Questions
M. tuberculosis and non-tuberculous mycobacteria
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app