
Thrombolysis inclusion/exclusion criteria — MCQs

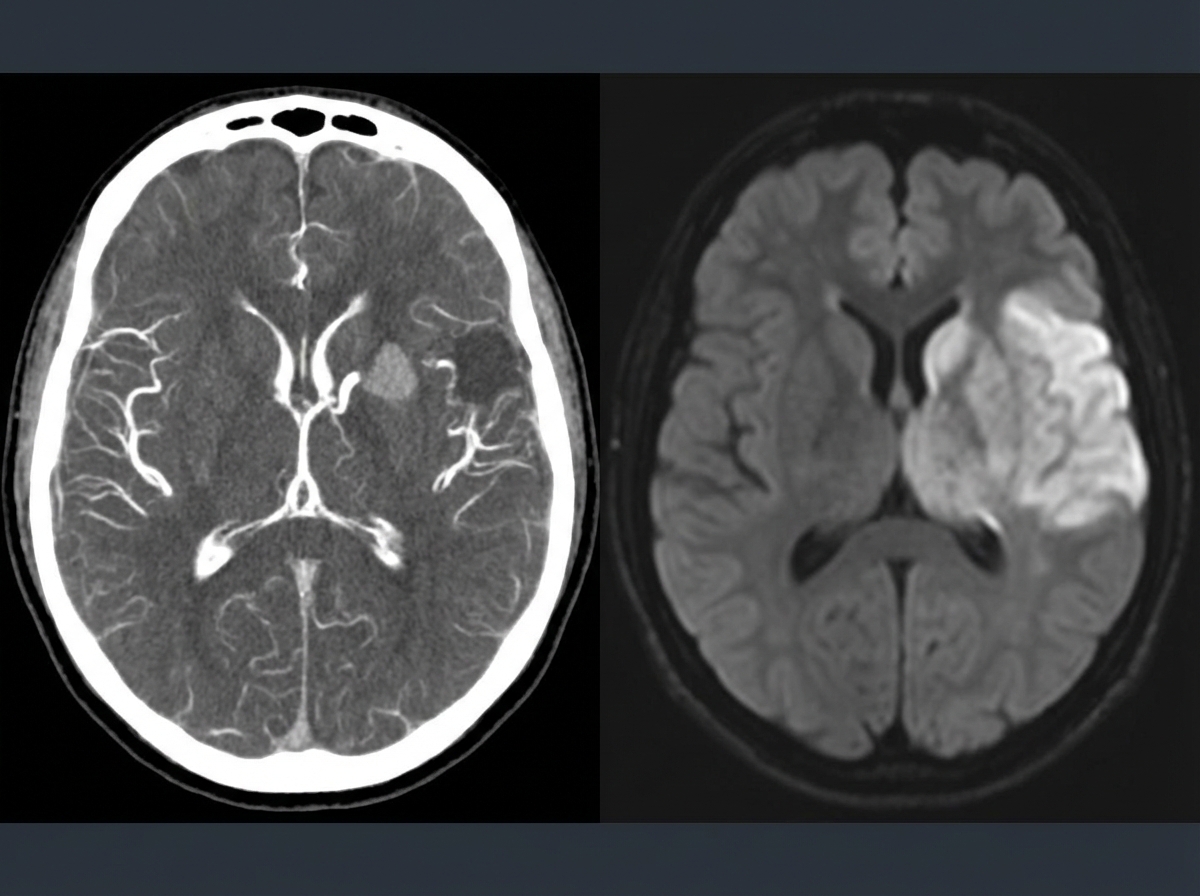
A 69-year-old man is brought in by his wife with acute onset aphasia for the past 5 hours. The patient's wife says that they were sitting having dinner when suddenly he was not able to speak. They delayed coming to the hospital because he had a similar episode 2 months ago which resolved within an hour. His past medical history is significant for hypercholesterolemia, managed with rosuvastatin, and a myocardial infarction (MI) 2 months ago, status post percutaneous transluminal coronary angioplasty complicated by residual angina. His family history is significant for his father who died of MI at age 60. The patient reports a 15-pack-year smoking history but denies any alcohol or recreational drug use. The vital signs include: temperature 37.0℃ (98.6℉), blood pressure 125/85 mm Hg, pulse 96/min, and respiratory rate 19/min. On physical examination, the patient has expressive aphasia. There is a weakness of the right-sided lower facial muscles. The strength in his upper and lower extremities is 4/5 on the right and 5/5 on the left. There is also a decreased sensation on his right side. A noncontrast computed tomography (CT) scan of the head is unremarkable. CT angiography (CTA) and diffusion-weighted magnetic resonance imaging (MRI) of the brain are acquired, and the findings are shown in the exhibit (see image). Which of the following is the best course of treatment in this patient?
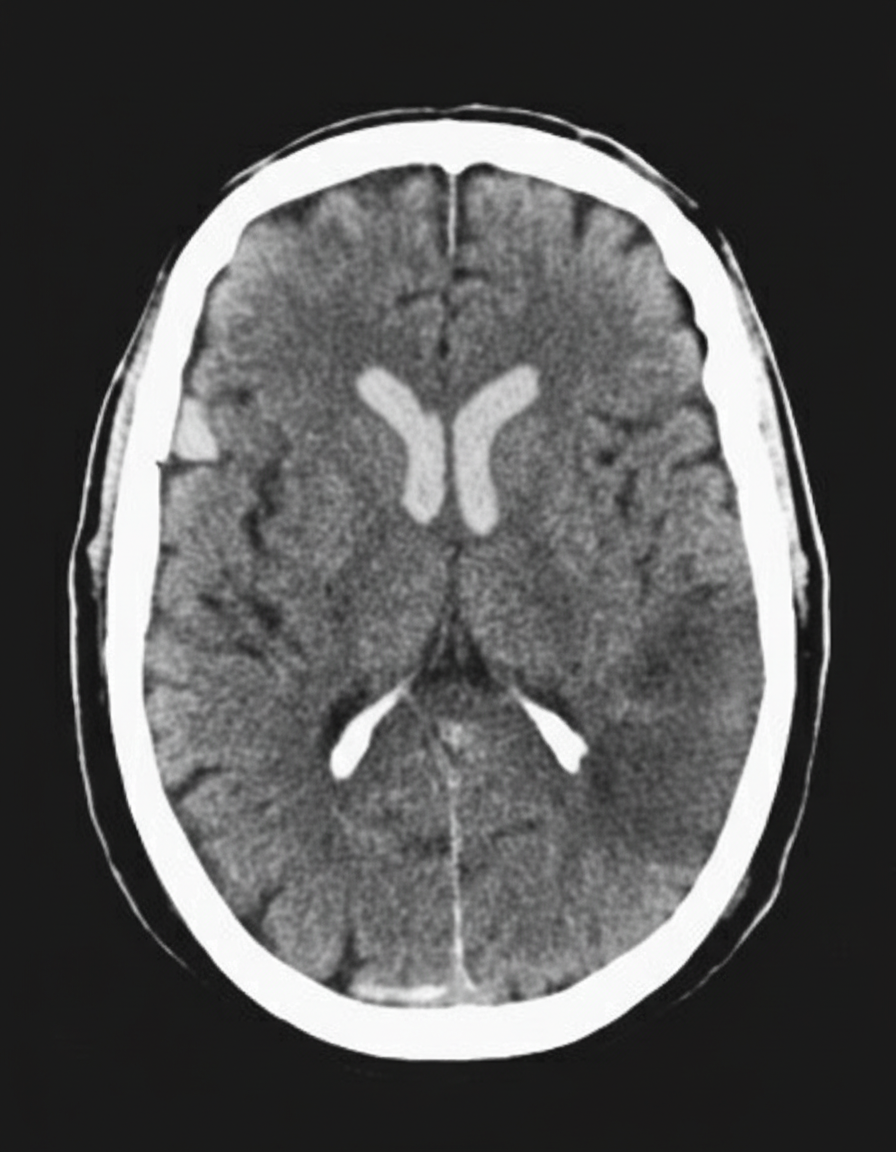
A 74-year-old man is rushed to the emergency department with left-sided weakness, facial deviation, and slurred speech. His wife first noticed these changes about an hour ago. The patient is having difficulty communicating. He can answer questions by nodding his head, and his wife is providing detailed information. He denies fever, loss of consciousness, head injury, bleeding, or seizures. Past medical history is significant for diabetes mellitus, hypertension, hyperlipidemia, ischemic heart disease, chronic kidney disease, and osteoarthritis. He had a heart attack 6 weeks ago. Baseline creatinine is 2.5 mg/dL, and he is not on hemodialysis. Medications include aspirin, clopidogrel, metoprolol, ramipril, rosuvastatin, and insulin detemir. Blood pressure is 175/95 mm Hg and the heart rate is 121/min. Muscle strength is decreased in both the upper and lower extremities on the left-side. A forehead sparing left sided facial weakness is also appreciated. An ECG reveals atrial fibrillation. An urgent head CT shows a hypodense area in the right parietal cortex with no indication of hemorrhage. Treatment with tissue plasminogen activator (tPA) is deferred due to which condition?
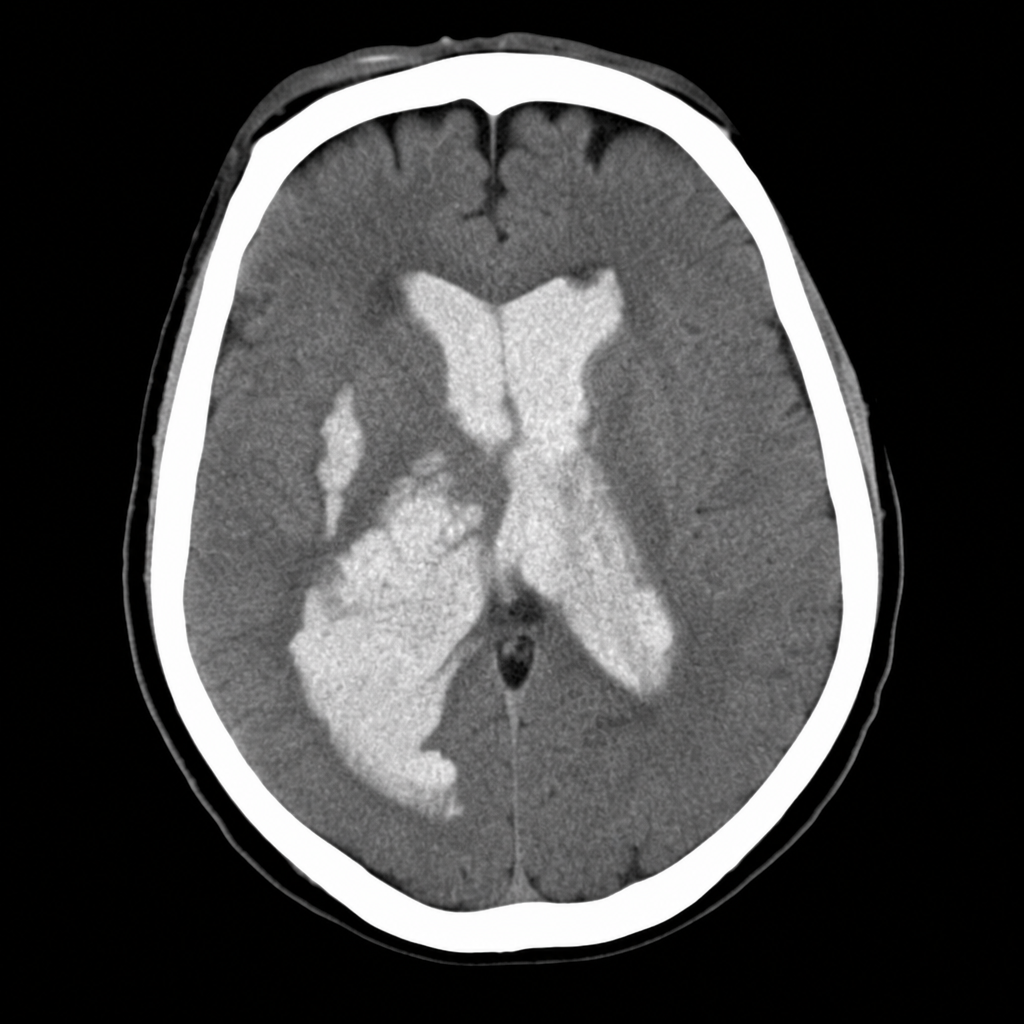
A 45-year-old man presents to the emergency department with complaints of right-sided weakness and slurring of speech for 1 hour. There is no history of head trauma, myocardial infarction, recent surgery, gastrointestinal or urinary bleeding. He has hypertension, chronic atrial fibrillation, and a 20 pack-year cigarette smoking history. The medication list includes valsartan and rivaroxaban. The vital signs include: blood pressure 180/92 mm Hg, pulse 144/min and irregular, and temperature 37.2°C (99.0°F). On physical examination, there is a facial asymmetry with a deviation of angle of mouth to the left side on smiling. Muscle strength is reduced in both upper and lower limbs on the right side while on the left side it’s normal. Random blood glucose is 104 mg/dL. A complete blood count is normal. A CT scan of the head is shown in the image. What is the most appropriate next step in the management of this patient?
A researcher is investigating the risk of symptomatic intracerebral hemorrhage associated with tissue plasminogen activator (tPA) treatment in severe ischemic stroke. The outcomes of a large randomized controlled trial of ischemic stroke patients, some of whom were randomized to tPA, is shown: Symptomatic intracerebral hemorrhage No symptomatic intracerebral hemorrhage Received tPA 12 188 Did not receive tPA 25 475 Based on this data, how many patients with severe ischemic stroke would need to be treated with tPA, on average, to contribute to one case of symptomatic intracerebral hemorrhage?
A 77-year-old woman is brought by ambulance to the emergency department after she developed weakness of her right arm along with a right-sided facial droop. By the time the ambulance arrived, she was having difficulty speaking. Past medical history is significant for hypertension, diabetes mellitus type II, and hyperlipidemia. She takes lisinopril, hydrochlorothiazide, metformin, and atorvastatin. On arrival to the emergency department, her vital signs are within normal limits. On physical examination, she is awake and alert but the right side of her mouth is dropping, making it difficult for her to speak clearly. Her heart has a regular rate and rhythm and her lungs are clear to auscultation bilaterally. Fingerstick glucose is 85 mg/dL. Her right upper extremity strength is 2/5 and her left upper extremity strength is 5/5. Which of the following is the best next step in management?
A 65-year-old man presents to the emergency department for sudden weakness. He was doing mechanical work on his car where he acutely developed right-leg weakness and fell to the ground. He is accompanied by his wife, who said that this has never happened before. He was last seen neurologically normal approximately 2 hours prior to presentation. His past medical history is significant for hypertension and type II diabetes. His temperature is 98.8°F (37.1°C), blood pressure is 177/108 mmHg, pulse is 90/min, respirations are 15/min, and oxygen saturation is 99% on room air. Neurological exam reveals that he is having trouble speaking and has profound weakness of his right upper and lower extremity. Which of the following is the best next step in management?
A 58-year-old woman is brought to the emergency department after sudden onset of the worst headache of her life followed by loss of consciousness. She is now obtunded with a GCS of 10. Vital signs: BP 192/110 mmHg, HR 96 bpm, SpO2 94% on room air. The emergency physician reviews the CT head image shown. Based on the imaging finding, which of the following is the most appropriate immediate management decision?
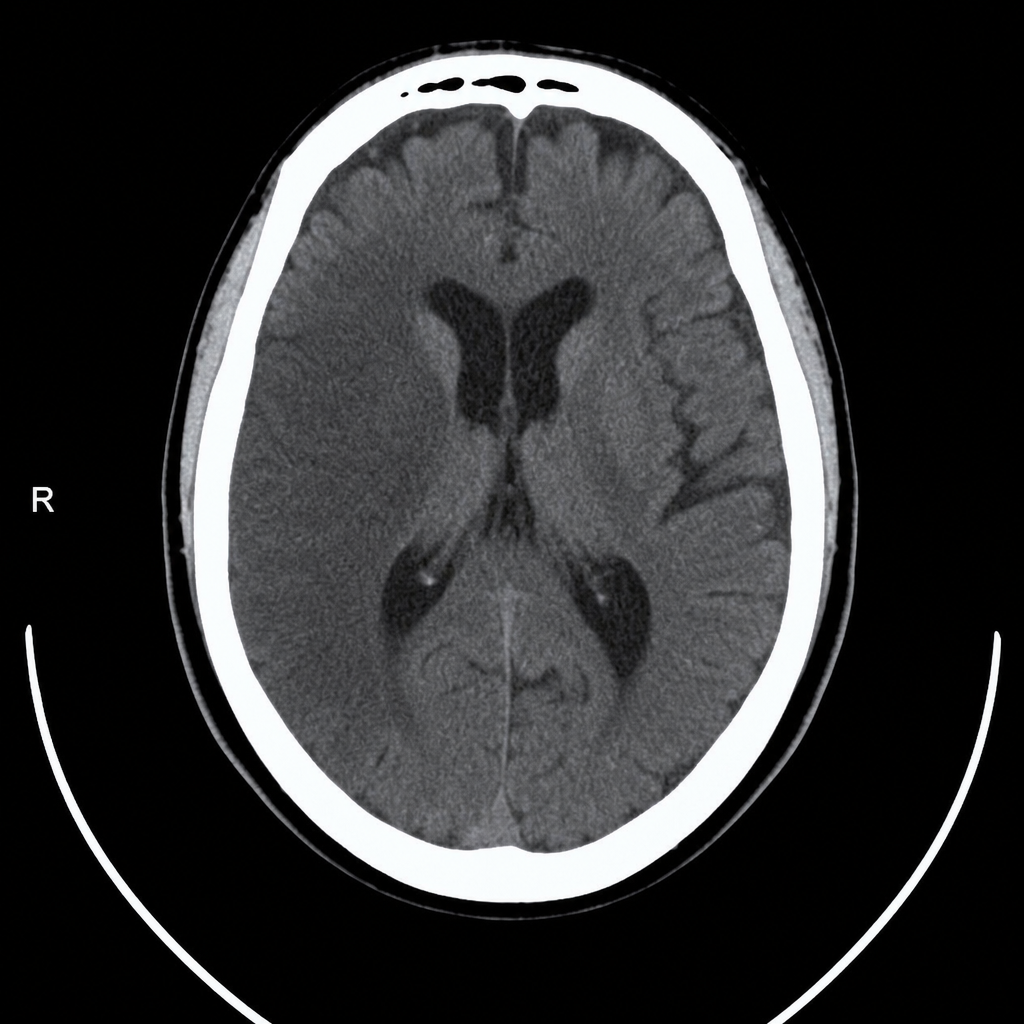
A 67-year-old man with hypertension and type 2 diabetes is brought to the emergency department by his wife, who noticed he was unable to lift his right arm and his speech became slurred 2 hours ago. Vital signs: BP 188/104 mmHg, HR 82 bpm, RR 16, SpO2 97% on room air. Neurological exam reveals right-sided facial droop, right arm weakness (2/5), and dysarthria; NIHSS score is 14. A non-contrast CT head is performed and reviewed. The image is shown above. His blood pressure must be controlled before alteplase can be given. Which of the following is the most appropriate next step in management?
A 48-year-old woman presents with acute stroke symptoms 18 hours ago. MRI shows a right MCA M1 occlusion with large penumbra on perfusion imaging (mismatch ratio >1.8) and small infarct core (25 mL). Her NIHSS is 16. She has no significant comorbidities. Her family is concerned about disability but wants to pursue treatment if reasonable chance of benefit exists. Synthesize the evidence and evaluate the treatment approach.
A 55-year-old man undergoes successful thrombectomy for left MCA occlusion. Post-procedure, he develops progressive lethargy and his blood pressure increases to 180/100 mmHg. CT shows hyperdensity in the treated territory without hemorrhage, and his symptoms worsen over 4 hours despite blood pressure control. Evaluate the most likely diagnosis and management priority.
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app