
Swallowing assessment and management — MCQs

A 58-year-old man comes to the physician for the evaluation of intermittent dysphagia for 6 months. He states that he drinks a lot of water during meals to help reduce discomfort he has while swallowing food. He has hypertension and gastroesophageal reflux disease. He has smoked one half-pack of cigarettes daily for 32 years. He does not drink alcohol. Current medications include hydrochlorothiazide and ranitidine. He is 173 cm (5 ft 8 in) tall and weighs 101 kg (222 lb); BMI is 33.7 kg/m2. His temperature is 37°C (98.6°F), pulse is 75/min, and blood pressure is 125/75 mm Hg. The lungs are clear to auscultation. Cardiac examination shows no murmurs, rubs, or gallops. The abdomen is soft and nontender. A barium esophagogram shows a smooth, circumferential narrowing at the distal esophagus. An upper endoscopy shows a sliding hiatal hernia and a thin mucosal ring at the gastroesophageal junction. Biopsies from the area show normal squamous and columnar epithelium with no dysplasia or malignancy. Which of the following is the most appropriate next step in the management of this patient?
A 49-year-old man presents to his primary care physician complaining of multiple symptoms. He states that over the past 8 months he has noticed voice changes and difficulty swallowing. The dysphagia started with just dry foods like crackers but has progressed to include smoothies and ice cream. He works as a newspaper editor and has also noticed trouble writing with his dominant hand. He is accompanied by his wife, who complains that he snores and drools in his sleep. His medical history is significant for hypertension and a bicuspid aortic valve. He takes hydrochlorothiazide. On physical examination, there is atrophy of the right hand. The patient’s speech is slow. A systolic murmur at the right upper sternal border is appreciated. Tapping of the left patellar tendon causes the patient’s left lower extremity to forcefully kick out. Stroking of the plantar aspect of the patient’s left foot causes his left toes to extend upward. Which of the following therapies is most likely to slow the progression of the patient’s symptoms?
A 55-year-old man presents to his primary care physician for trouble swallowing. The patient claims that he used to struggle when eating food if he did not chew it thoroughly, but now he occasionally struggles with liquids as well. He also complains of a retrosternal burning sensation whenever he eats. He also claims that he feels his throat burns when he lays down or goes to bed. Otherwise, the patient has no other complaints. The patient has a past medical history of obesity, diabetes, constipation, and anxiety. His current medications include insulin, metformin, and lisinopril. On review of systems, the patient endorses a 5 pound weight loss recently. The patient has a 22 pack-year smoking history and drinks alcohol with dinner. His temperature is 99.5°F (37.5°C), blood pressure is 177/98 mmHg, pulse is 90/min, respirations are 17/min, and oxygen saturation is 98% on room air. On physical exam, you note an overweight man in no current distress. Abdominal exam is within normal limits. Which of the following is the best next step in management?
A 72-year-old man is admitted to the hospital because of a 2-day history of right-sided weakness and dysphagia. He is diagnosed with a thrombotic stroke and treatment with aspirin is initiated. A videofluoroscopic swallowing study is performed to determine his ability to swallow safely; he is found to be at increased risk of aspiration. Consequently, he is ordered not to have any food or liquids by mouth. A Dobhoff feeding tube is placed, tube feedings are ordered, and the patient starts receiving tube feedings. Shortly after, he develops a cough and dyspnea. An x-ray of the chest shows opacification of the right lower lobe and that the end of the Dobhoff tube is in his right lung instead of his stomach. Which of the following would most likely have prevented this medical error from occurring?
A 73-year-old man comes to the physician because of a 4-kg (9-lb) weight loss over the last month. During this time he has not been able to eat more than one bite without coughing immediately and sometimes he regurgitates food through his nose. His symptoms are worse with liquids. One month ago he had a stroke in the right middle cerebral artery. He has a history of hypertension, type 2 diabetes mellitus, and hyperlipidemia. Current medications include aspirin, amlodipine, metformin, and simvastatin. Examination of the oropharynx, chest, and abdomen shows no abnormalities. Neurological examination shows facial drooping on the left and decreased strength in the left upper and lower extremities. Which of the following is the most appropriate next step in management?
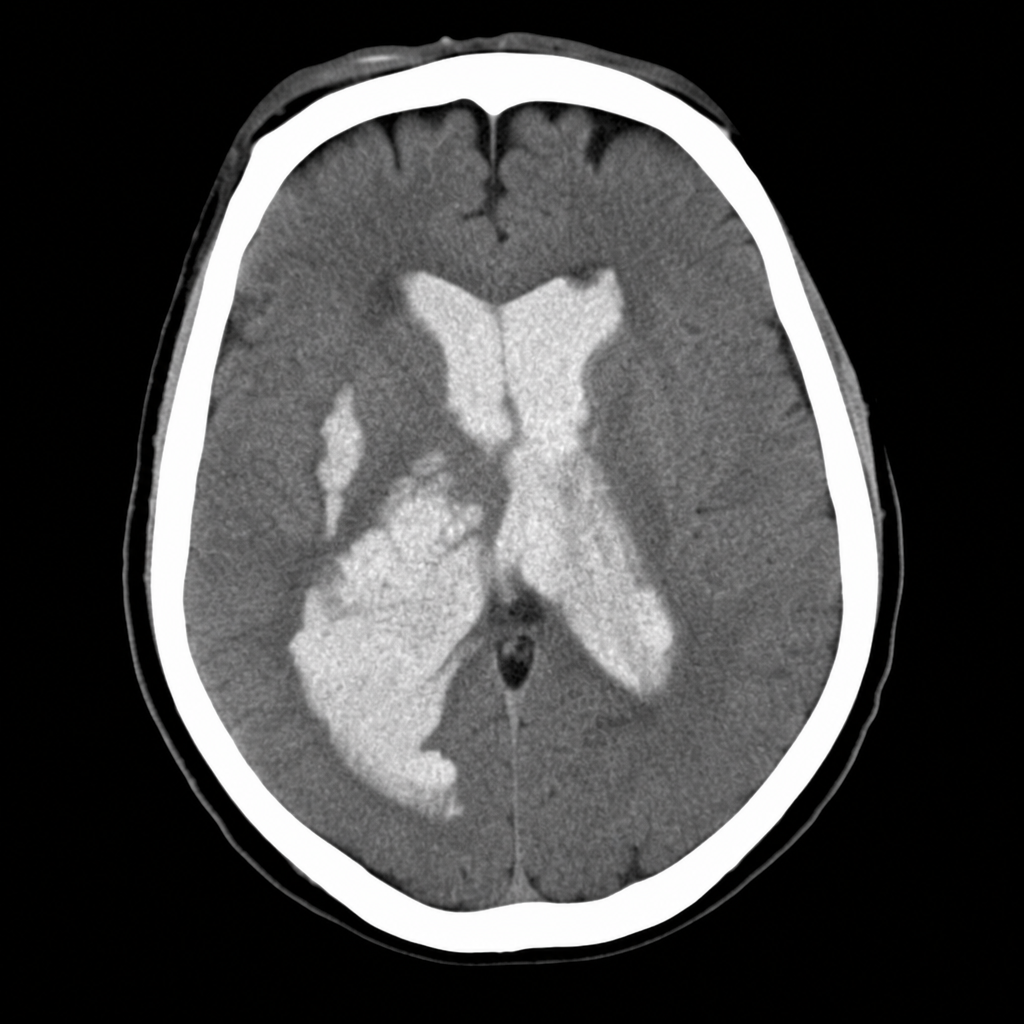
A 58-year-old woman is brought to the emergency department after sudden onset of the worst headache of her life followed by loss of consciousness. She is now obtunded with a GCS of 10. Vital signs: BP 192/110 mmHg, HR 96 bpm, SpO2 94% on room air. The emergency physician reviews the CT head image shown. Based on the imaging finding, which of the following is the most appropriate immediate management decision?
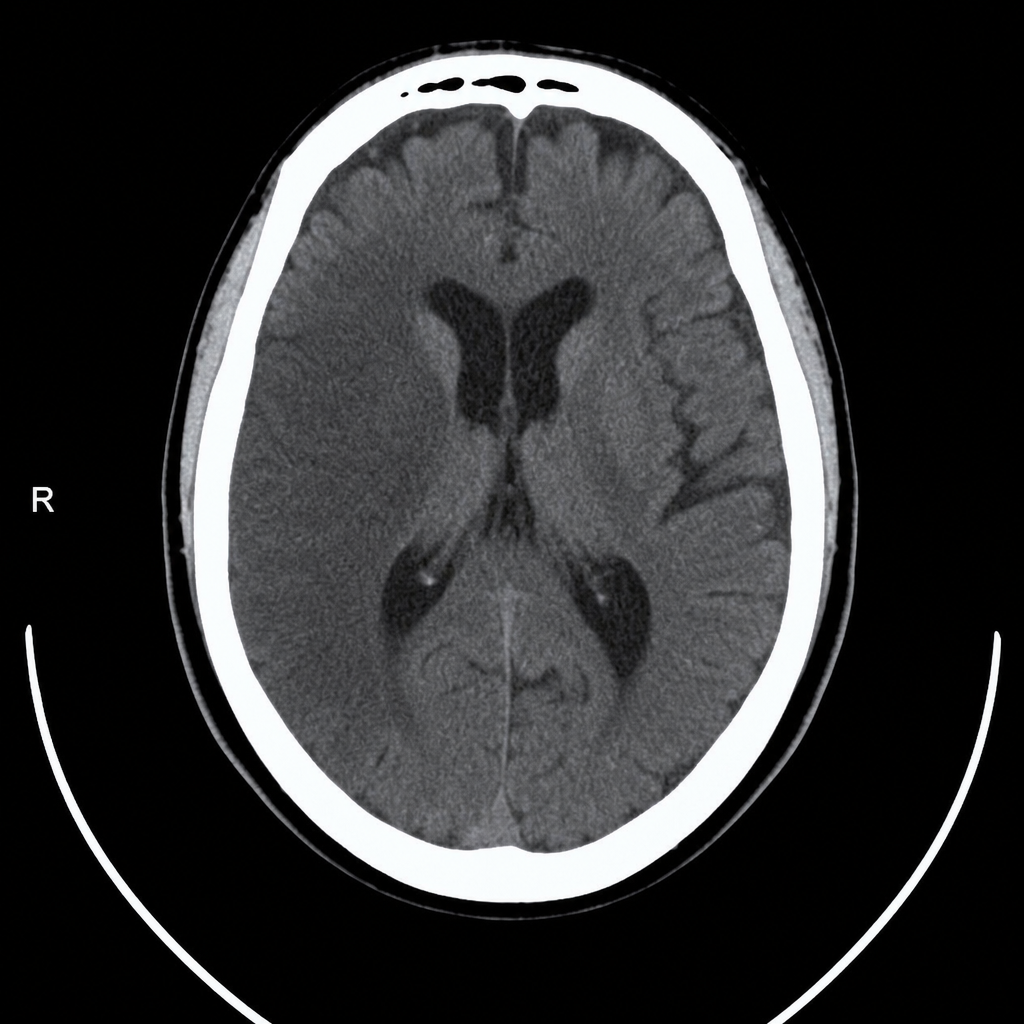
A 67-year-old man with hypertension and type 2 diabetes is brought to the emergency department by his wife, who noticed he was unable to lift his right arm and his speech became slurred 2 hours ago. Vital signs: BP 188/104 mmHg, HR 82 bpm, RR 16, SpO2 97% on room air. Neurological exam reveals right-sided facial droop, right arm weakness (2/5), and dysarthria; NIHSS score is 14. A non-contrast CT head is performed and reviewed. The image is shown above. His blood pressure must be controlled before alteplase can be given. Which of the following is the most appropriate next step in management?
A 48-year-old woman presents with acute stroke symptoms 18 hours ago. MRI shows a right MCA M1 occlusion with large penumbra on perfusion imaging (mismatch ratio >1.8) and small infarct core (25 mL). Her NIHSS is 16. She has no significant comorbidities. Her family is concerned about disability but wants to pursue treatment if reasonable chance of benefit exists. Synthesize the evidence and evaluate the treatment approach.
A 55-year-old man undergoes successful thrombectomy for left MCA occlusion. Post-procedure, he develops progressive lethargy and his blood pressure increases to 180/100 mmHg. CT shows hyperdensity in the treated territory without hemorrhage, and his symptoms worsen over 4 hours despite blood pressure control. Evaluate the most likely diagnosis and management priority.
An 80-year-old woman with atrial fibrillation presents 2 hours after acute ischemic stroke. NIHSS is 22. Imaging shows large left MCA territory infarction involving >1/3 of MCA territory with basilar artery occlusion. She lives alone but was independent before this event. Her family requests all possible interventions. Evaluate the management approach considering benefits versus risks.
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app