
Stroke unit care principles — MCQs

A 15-year-old boy is brought to the emergency department one hour after sustaining an injury during football practice. He collided head-on into another player while wearing a mouthguard and helmet. Immediately after the collision he was confused but able to use appropriate words. He opened his eyes spontaneously and followed commands. There was no loss of consciousness. He also had a headache with dizziness and nausea. He is no longer confused upon arrival. He feels well. Vital signs are within normal limits. He is fully alert and oriented. His speech is organized and he is able to perform tasks demonstrating full attention, memory, and balance. Neurological examination shows no abnormalities. There is mild tenderness to palpation over the crown of his head but no signs of skin break or fracture. Which of the following is the most appropriate next step?
A recent study examined trends in incidence and fatality of ischemic stroke in a representative sample of Scandinavian towns. The annual incidence of ischemic stroke was calculated to be 60 per 2,000 people. The 1-year case fatality rate for ischemic stroke was found to be 20%. The health department of a town in southern Sweden with a population of 20,000 is interested in knowing the 1-year mortality conferred by ischemic stroke. Based on the study's findings, which of the following estimates the annual mortality rate for ischemic stroke per 20,000?
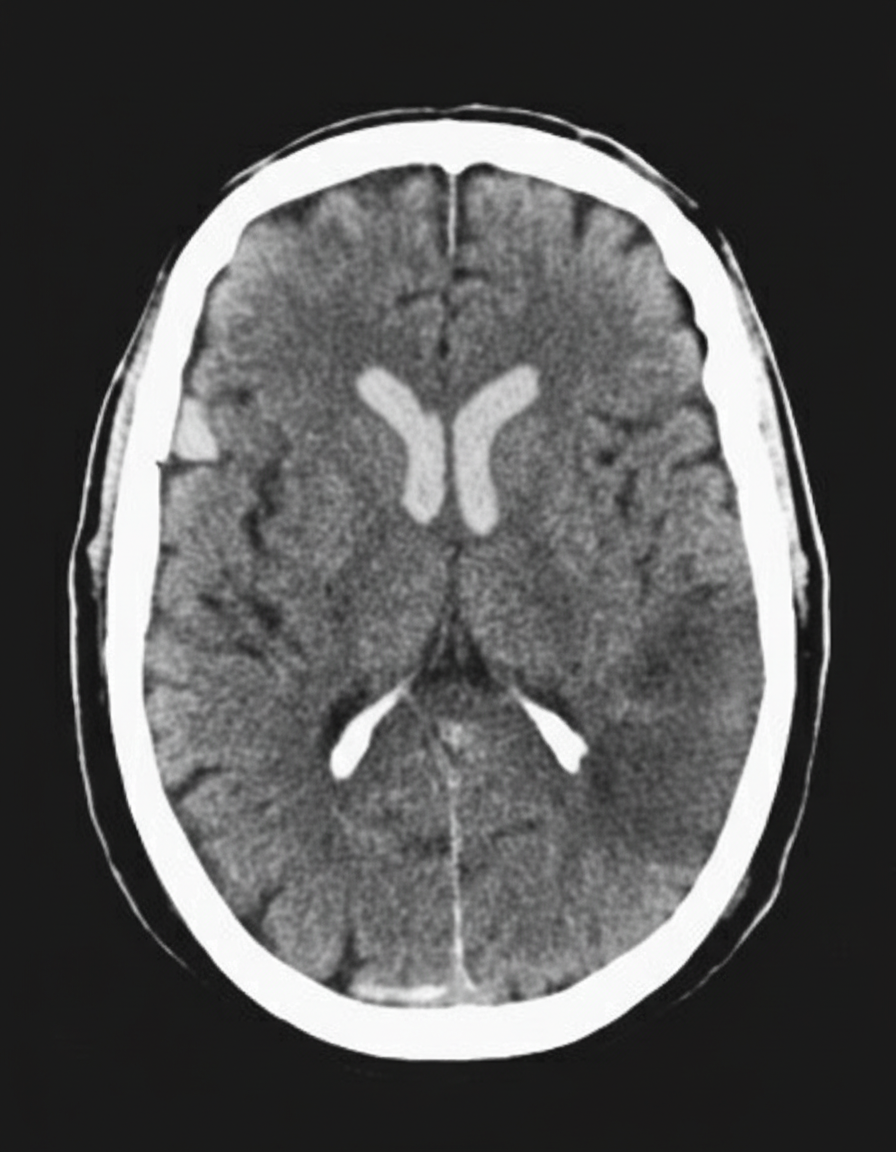
A 45-year-old man presents to the emergency department with complaints of right-sided weakness and slurring of speech for 1 hour. There is no history of head trauma, myocardial infarction, recent surgery, gastrointestinal or urinary bleeding. He has hypertension, chronic atrial fibrillation, and a 20 pack-year cigarette smoking history. The medication list includes valsartan and rivaroxaban. The vital signs include: blood pressure 180/92 mm Hg, pulse 144/min and irregular, and temperature 37.2°C (99.0°F). On physical examination, there is a facial asymmetry with a deviation of angle of mouth to the left side on smiling. Muscle strength is reduced in both upper and lower limbs on the right side while on the left side it’s normal. Random blood glucose is 104 mg/dL. A complete blood count is normal. A CT scan of the head is shown in the image. What is the most appropriate next step in the management of this patient?
A 69-year-old male presents to the emergency department for slurred speech and an inability to use his right arm which occurred while he was eating dinner. The patient arrived at the emergency department within one hour. A CT scan was performed of the head and did not reveal any signs of hemorrhage. The patient is given thrombolytics and is then managed on the neurology floor. Three days later, the patient is recovering and is stable. He seems depressed but is doing well with his symptoms gradually improving as compared to his initial presentation. The patient complains of neck pain that has worsened slowly over the past few days for which he is being given ibuprofen. Laboratory values are ordered and return as indicated below: Serum: Na+: 130 mEq/L K+: 3.7 mEq/L Cl-: 100 mEq/L HCO3-: 24 mEq/L Urea nitrogen: 7 mg/dL Glucose: 70 mg/dL Creatinine: 0.9 mg/dL Ca2+: 9.7 mg/dL Urine: Appearance: dark Glucose: negative WBC: 0/hpf Bacterial: none Na+: 320 mEq/L/24 hours His temperature is 99.5°F (37.5°C), pulse is 95/min, blood pressure is 129/70 mmHg, respirations are 10/min, and oxygen saturation is 98% on room air. Which of the following is the best next step in management?
A 78-year-old man is brought in to the emergency department by ambulance after his wife noticed that he began slurring his speech and had developed facial asymmetry during dinner approximately 30 minutes ago. His past medical history is remarkable for hypertension and diabetes. His temperature is 99.1°F (37.3°C), blood pressure is 154/99 mmHg, pulse is 89/min, respirations are 12/min, and oxygen saturation is 98% on room air. Neurologic exam reveals right upper and lower extremity weakness and an asymmetric smile. Which of the following is the next best step in management?
A 57-year-old man was brought into the emergency department unconscious 2 days ago. His friends who were with him at that time say he collapsed on the street. Upon arrival to the ED, he had a generalized tonic seizure. At that time, he was intubated and is being treated with diazepam and phenytoin. A noncontrast head CT revealed hemorrhages within the pons and cerebellum with a mass effect and tonsillar herniation. Today, his blood pressure is 110/65 mm Hg, heart rate is 65/min, respiratory rate is 12/min (intubated, ventilator settings: tidal volume (TV) 600 ml, positive end-expiratory pressure (PEEP) 5 cm H2O, and FiO2 40%), and temperature is 37.0°C (98.6°F). On physical examination, the patient is in a comatose state. Pupils are 4 mm bilaterally and unresponsive to light. Cornea reflexes are absent. Gag reflex and cough reflex are also absent. Which of the following is the next best step in the management of this patient?
A 5-year-old boy is brought to the emergency department by his mother because of a 2-hour history of word-finding difficulty, speech slurring, and weakness and sensory loss of his right arm and leg. He has not had fever, nausea, headache, or diarrhea. His mother reports an episode of severe pain and soft tissue swelling of the dorsum of his hands and feet when he was 12 months old, which self-resolved after 2 weeks. His temperature is 37.7°C (99.8°F), pulse is 90/min, and blood pressure is 110/80 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 91%. He follows commands but has nonfluent aphasia. Examination shows marked weakness and decreased sensation of the right upper and lower extremities. Deep tendon reflexes are 2+ bilaterally. Babinski sign is present on the right. An MRI scan of the brain shows signs of an evolving cerebral infarction on the patient's left side. Which of the following is the most appropriate initial step in management?
A 65-year-old man presents to the emergency department for sudden weakness. He was doing mechanical work on his car where he acutely developed right-leg weakness and fell to the ground. He is accompanied by his wife, who said that this has never happened before. He was last seen neurologically normal approximately 2 hours prior to presentation. His past medical history is significant for hypertension and type II diabetes. His temperature is 98.8°F (37.1°C), blood pressure is 177/108 mmHg, pulse is 90/min, respirations are 15/min, and oxygen saturation is 99% on room air. Neurological exam reveals that he is having trouble speaking and has profound weakness of his right upper and lower extremity. Which of the following is the best next step in management?
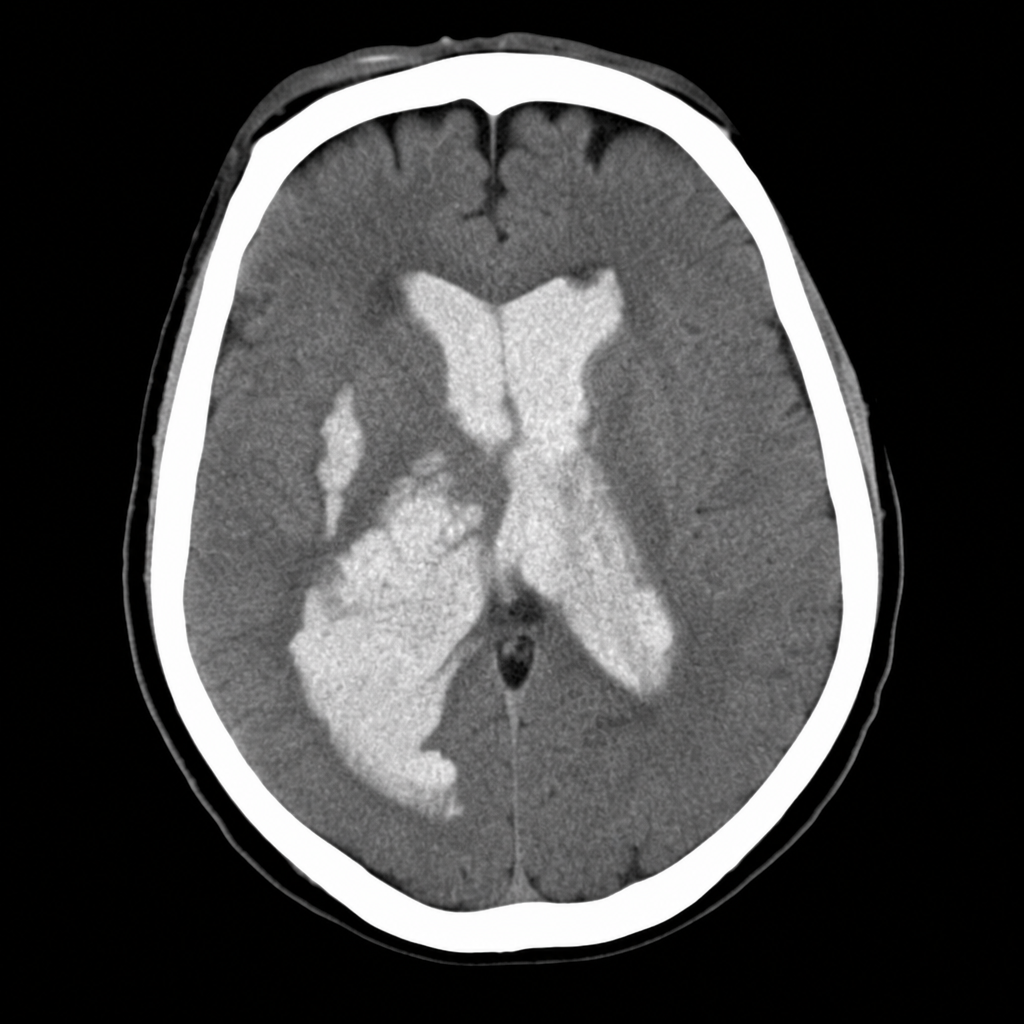
A 58-year-old woman is brought to the emergency department after sudden onset of the worst headache of her life followed by loss of consciousness. She is now obtunded with a GCS of 10. Vital signs: BP 192/110 mmHg, HR 96 bpm, SpO2 94% on room air. The emergency physician reviews the CT head image shown. Based on the imaging finding, which of the following is the most appropriate immediate management decision?
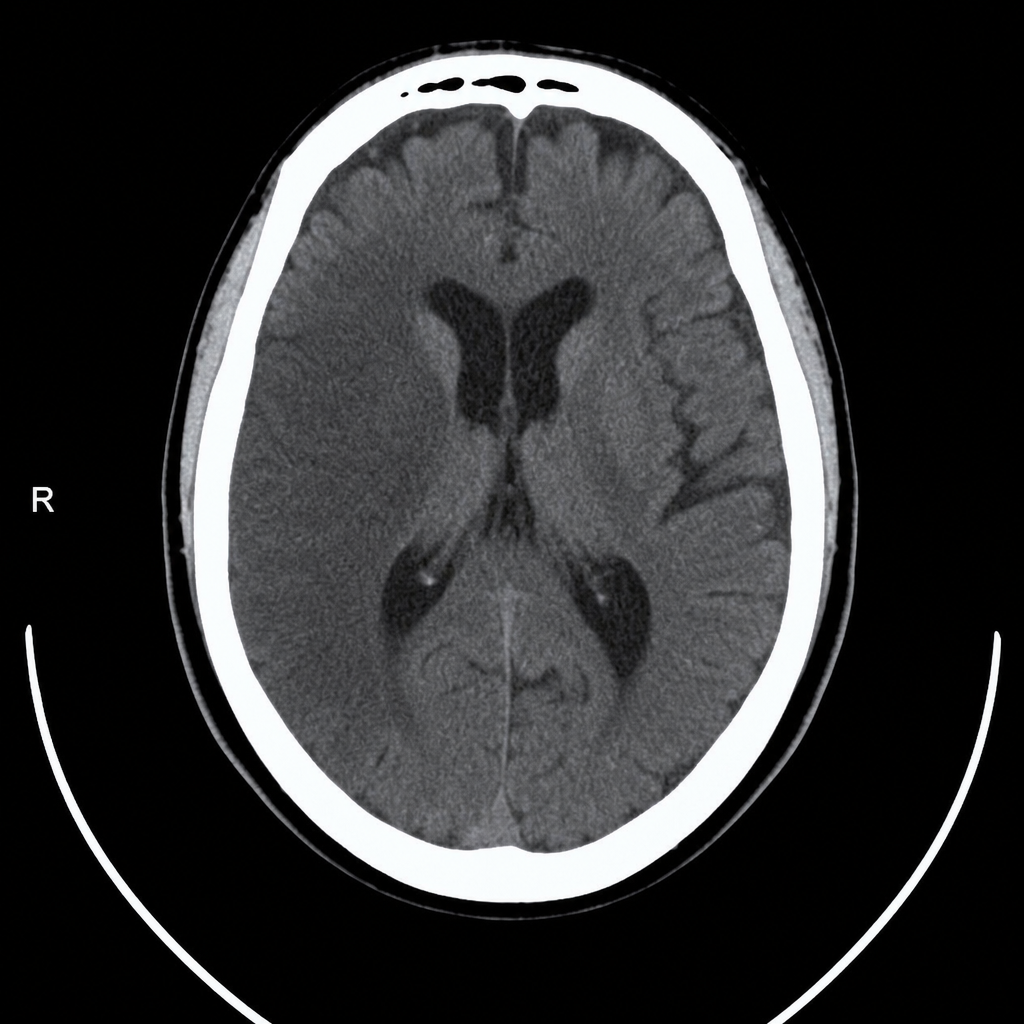
A 67-year-old man with hypertension and type 2 diabetes is brought to the emergency department by his wife, who noticed he was unable to lift his right arm and his speech became slurred 2 hours ago. Vital signs: BP 188/104 mmHg, HR 82 bpm, RR 16, SpO2 97% on room air. Neurological exam reveals right-sided facial droop, right arm weakness (2/5), and dysarthria; NIHSS score is 14. A non-contrast CT head is performed and reviewed. The image is shown above. His blood pressure must be controlled before alteplase can be given. Which of the following is the most appropriate next step in management?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app