
Rehabilitation principles — MCQs

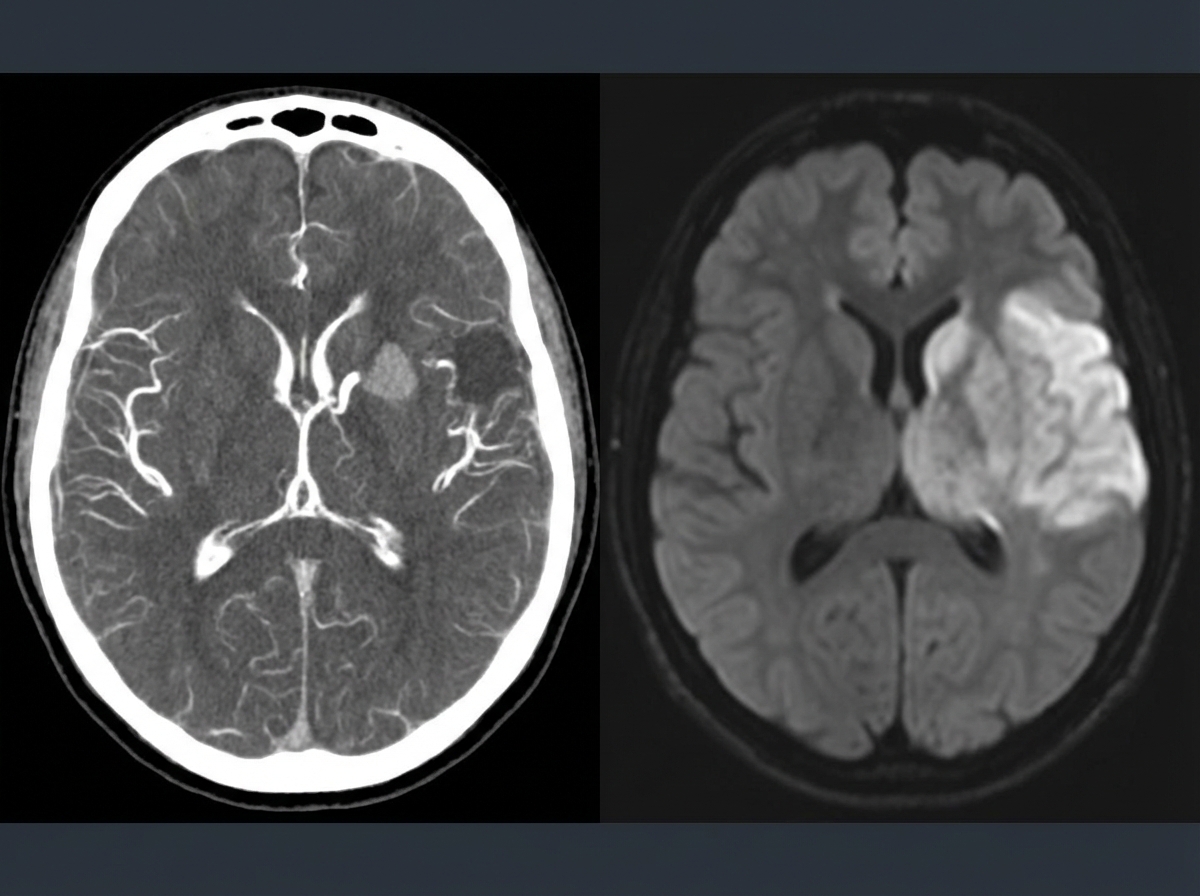
A 69-year-old man is brought in by his wife with acute onset aphasia for the past 5 hours. The patient's wife says that they were sitting having dinner when suddenly he was not able to speak. They delayed coming to the hospital because he had a similar episode 2 months ago which resolved within an hour. His past medical history is significant for hypercholesterolemia, managed with rosuvastatin, and a myocardial infarction (MI) 2 months ago, status post percutaneous transluminal coronary angioplasty complicated by residual angina. His family history is significant for his father who died of MI at age 60. The patient reports a 15-pack-year smoking history but denies any alcohol or recreational drug use. The vital signs include: temperature 37.0℃ (98.6℉), blood pressure 125/85 mm Hg, pulse 96/min, and respiratory rate 19/min. On physical examination, the patient has expressive aphasia. There is a weakness of the right-sided lower facial muscles. The strength in his upper and lower extremities is 4/5 on the right and 5/5 on the left. There is also a decreased sensation on his right side. A noncontrast computed tomography (CT) scan of the head is unremarkable. CT angiography (CTA) and diffusion-weighted magnetic resonance imaging (MRI) of the brain are acquired, and the findings are shown in the exhibit (see image). Which of the following is the best course of treatment in this patient?
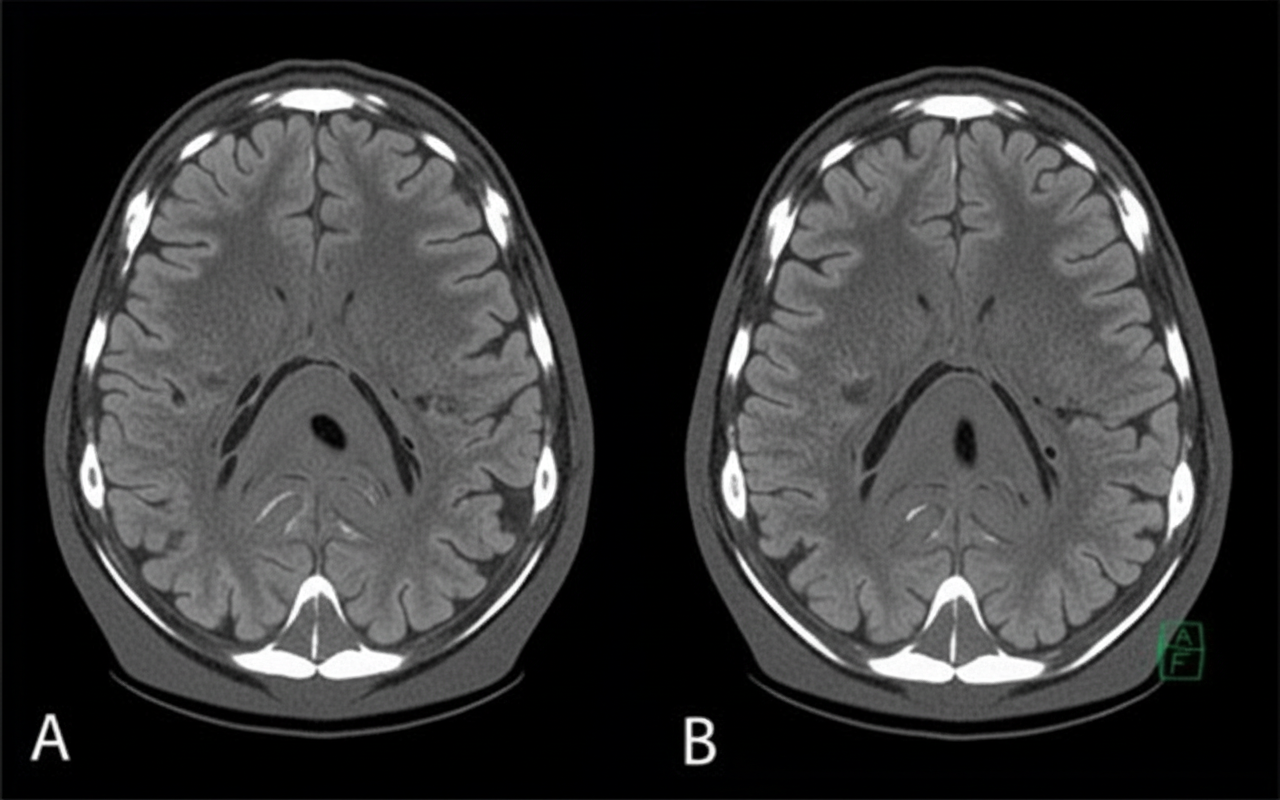
A 58-year-old man presents to the clinic concerned about his health after his elder brother recently became bed-bound due to a brain condition. He has also brought a head CT scan of his brother to reference, as shown in the picture. The patient has type 2 diabetes mellitus, hypertension, osteoarthritis, and hypercholesterolemia. His medication list includes aspirin, diclofenac sodium, metformin, and ramipril. He leads a sedentary lifestyle and smokes one pack of cigarettes daily. He also drinks 4–5 cups of red wine every weekend. His BMI is 33.2 kg/m2. His blood pressure is 164/96 mm Hg, the heart rate is 84/min, and the respiratory rate is 16/min. Which of the following interventions will be most beneficial for reducing the risk of developing the disease that his brother has?
A 68-year-old woman is brought to the emergency department by her husband because of acute confusion and sudden weakness of her left leg that lasted for about 30 minutes. One hour prior to admission, she was unable to understand words and had slurred speech for about 15 minutes. She has type 2 diabetes mellitus and hypertension. She has smoked 1 pack of cigarettes daily for 30 years. Current medications include metformin and hydrochlorothiazide. Her pulse is 110/min and irregular; blood pressure is 135/84 mmHg. Examination shows cold extremities. There is a mild bruit heard above the left carotid artery. Cardiac examination shows a grade 2/6 late systolic ejection murmur that begins with a midsystolic click. Neurological and mental status examinations show no abnormalities. An ECG shows irregularly spaced QRS complexes with no discernible P waves. Doppler ultrasonography shows mild left carotid artery stenosis. A CT scan and diffusion-weighted MRI of the brain show no abnormalities. Which of the following treatments is most likely to prevent future episodes of neurologic dysfunction in this patient?
A 4-year-old boy is brought to the physician because of non-fluent speech. His mother worries that his vocabulary is limited for his age and because he cannot use simple sentences to communicate. She says he enjoys playing with his peers and parents, but he has always lagged behind in his speaking and communication. His speech is frequently not understood by strangers. He physically appears normal. His height and weight are within the normal range for his age. He responds to his name, makes eye contact, and enjoys the company of his mother. Which of the following is the most appropriate next step in management?
A psychiatrist receives a call from a patient who expresses thoughts of harming his ex-girlfriend. The patient describes a detailed plan to attack her at her workplace. Which of the following represents the psychiatrist's most appropriate legal obligation?
A 78-year-old woman is accompanied by her family for a routine visit to her primary care provider. The family states that 5 months prior, the patient had a stroke and is currently undergoing physical therapy. Today, her temperature is 98.2°F (36.8°C), blood pressure is 112/72 mmHg, pulse is 64/min, and respirations are 12/min. On exam, she is alert and oriented with no deficits in speech. Additionally, her strength and sensation are symmetric and preserved bilaterally. However, on further neurologic testing, she appears to have some difficulty with balance and a propensity to fall to her right side. Which of the following deficits does the patient also likely have?
A 78-year-old man is brought in to the emergency department by ambulance after his wife noticed that he began slurring his speech and had developed facial asymmetry during dinner approximately 30 minutes ago. His past medical history is remarkable for hypertension and diabetes. His temperature is 99.1°F (37.3°C), blood pressure is 154/99 mmHg, pulse is 89/min, respirations are 12/min, and oxygen saturation is 98% on room air. Neurologic exam reveals right upper and lower extremity weakness and an asymmetric smile. Which of the following is the next best step in management?
A 73-year-old man is brought to the emergency department by ambulance after being found to be non-communicative by his family during dinner. On presentation he appears to be alert, though he is confused and cannot follow instructions. When he tries to speak, he vocalizes a string of fluent but unintelligible syllables. Given this presentation, his physician decides to administer tissue plasminogen activator to this patient. This intervention best represents which of the following principles?
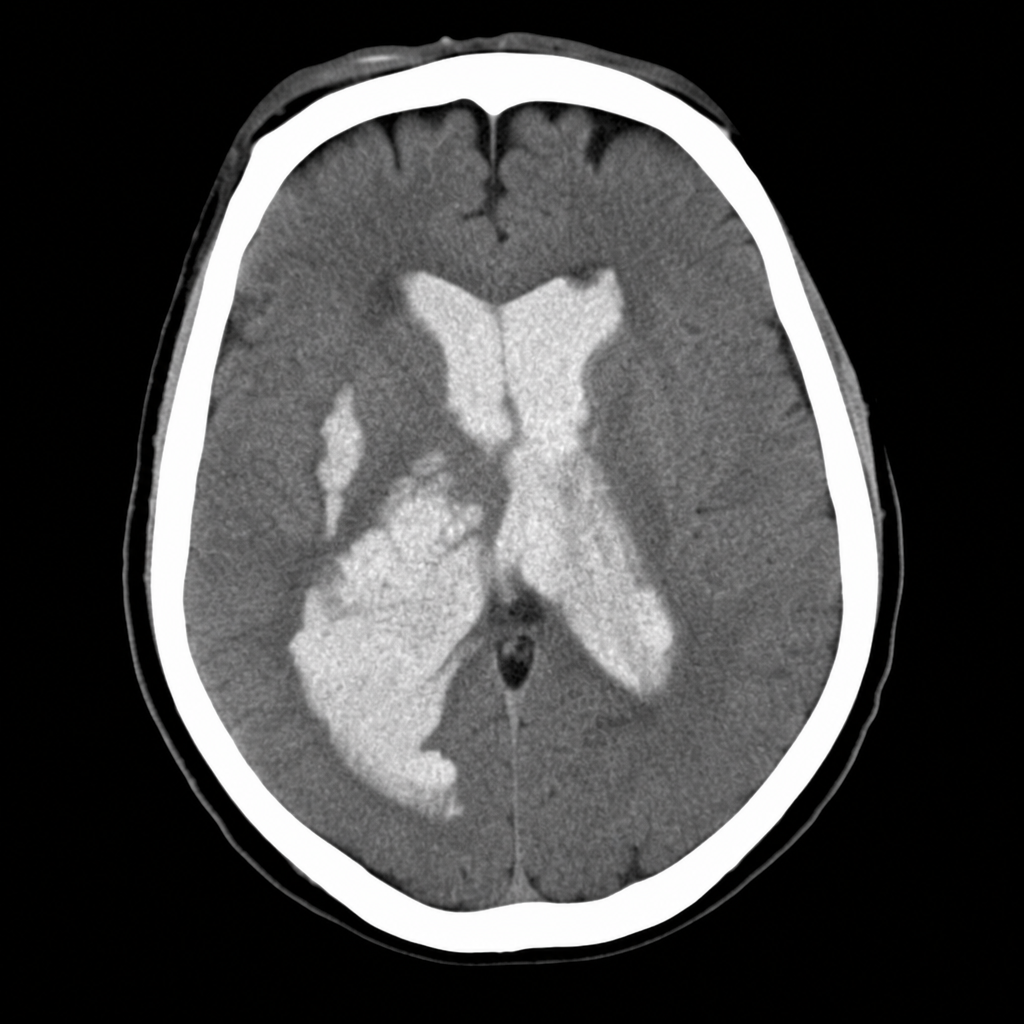
A 58-year-old woman is brought to the emergency department after sudden onset of the worst headache of her life followed by loss of consciousness. She is now obtunded with a GCS of 10. Vital signs: BP 192/110 mmHg, HR 96 bpm, SpO2 94% on room air. The emergency physician reviews the CT head image shown. Based on the imaging finding, which of the following is the most appropriate immediate management decision?
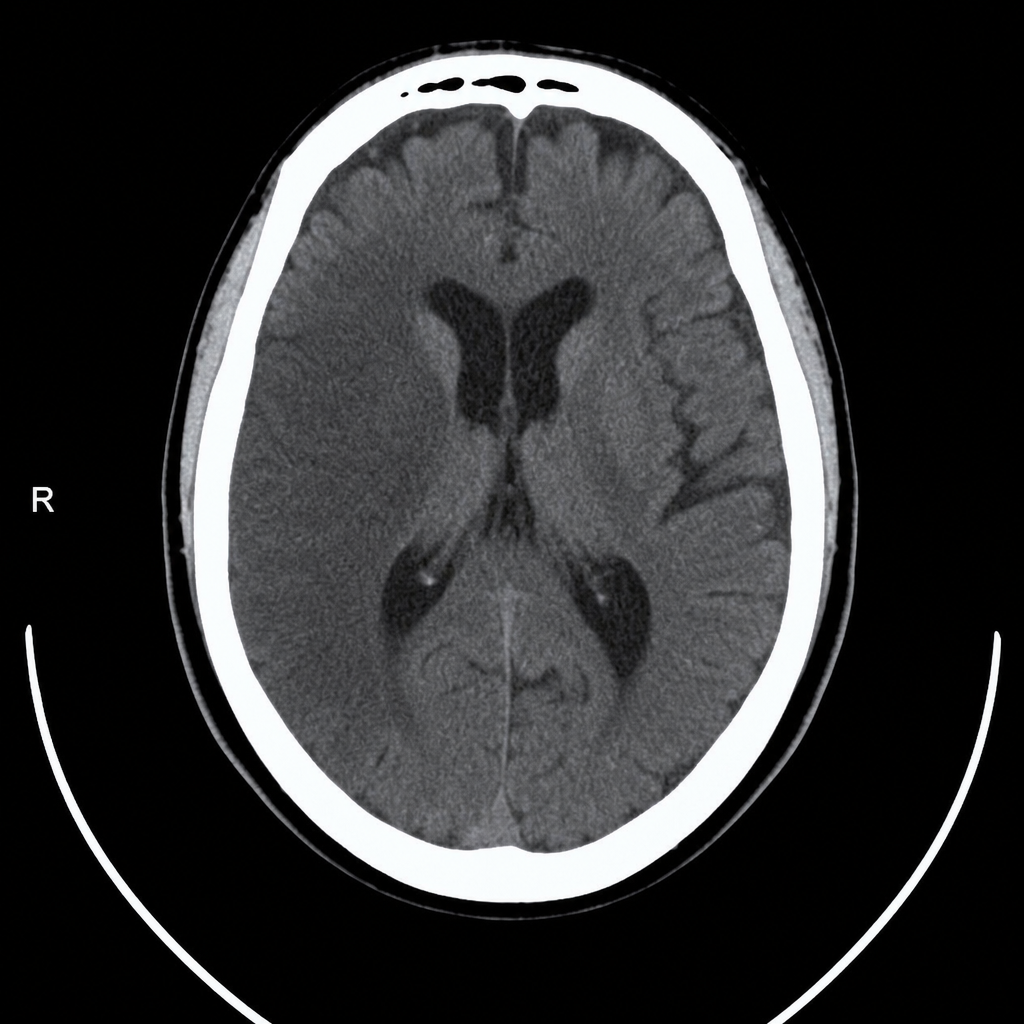
A 67-year-old man with hypertension and type 2 diabetes is brought to the emergency department by his wife, who noticed he was unable to lift his right arm and his speech became slurred 2 hours ago. Vital signs: BP 188/104 mmHg, HR 82 bpm, RR 16, SpO2 97% on room air. Neurological exam reveals right-sided facial droop, right arm weakness (2/5), and dysarthria; NIHSS score is 14. A non-contrast CT head is performed and reviewed. The image is shown above. His blood pressure must be controlled before alteplase can be given. Which of the following is the most appropriate next step in management?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app