
Mechanical thrombectomy indications — MCQs

A researcher is investigating the risk of symptomatic intracerebral hemorrhage associated with tissue plasminogen activator (tPA) treatment in severe ischemic stroke. The outcomes of a large randomized controlled trial of ischemic stroke patients, some of whom were randomized to tPA, is shown: Symptomatic intracerebral hemorrhage No symptomatic intracerebral hemorrhage Received tPA 12 188 Did not receive tPA 25 475 Based on this data, how many patients with severe ischemic stroke would need to be treated with tPA, on average, to contribute to one case of symptomatic intracerebral hemorrhage?
A 6-month-old male presents to the emergency department with his parents after his three-year-old brother hit him on the arm with a toy truck. His parents are concerned that the minor trauma caused an unusual amount of bruising. The patient has otherwise been developing well and meeting all his milestones. His parents report that he sleeps throughout the night and has just started to experiment with solid food. The patient’s older brother is in good health, but the patient’s mother reports that some members of her family have an unknown blood disorder. On physical exam, the patient is agitated and difficult to soothe. He has 2-3 inches of ecchymoses and swelling on the lateral aspect of the left forearm. The patient has a neurological exam within normal limits and pale skin with blue irises. An ophthalmologic evaluation is deferred. Which of the following is the best initial step?
A 60-year-old male is admitted to the ICU for severe hypertension complicated by a headache. The patient has a past medical history of insulin-controlled diabetes, hypertension, and hyperlipidemia. He smokes 2 packs of cigarettes per day. He states that he forgot to take his medications yesterday and started getting a headache about one hour ago. His vitals on admission are the following: blood pressure of 160/110 mmHg, pulse 95/min, temperature 98.6 deg F (37.2 deg C), and respirations 20/min. On exam, the patient has an audible abdominal bruit. After administration of antihypertensive medications, the patient has a blood pressure of 178/120 mmHg. The patient reports his headache has increased to a 10/10 pain level, that he has trouble seeing, and he can't move his extremities. After stabilizing the patient, what is the best next step to diagnose the patient's condition?
A 78-year-old man is brought in to the emergency department by ambulance after his wife noticed that he began slurring his speech and had developed facial asymmetry during dinner approximately 30 minutes ago. His past medical history is remarkable for hypertension and diabetes. His temperature is 99.1°F (37.3°C), blood pressure is 154/99 mmHg, pulse is 89/min, respirations are 12/min, and oxygen saturation is 98% on room air. Neurologic exam reveals right upper and lower extremity weakness and an asymmetric smile. Which of the following is the next best step in management?
A 30-year-old man with history of intravenous drug use and methamphetamine-associated chronic thromboembolic pulmonary hypertension (CTEPH) is brought to the emergency department by his girlfriend for worsening abdominal pain and fevers. The patient said the pain was initially around his umbilicus, but he is now experiencing intense tenderness near his groin. He was initially prescribed rivaroxaban, but due to insurance issues, he was switched to warfarin for management of CTEPH two weeks ago. His temperature is 102°F (38.9°C), blood pressure is 95/60 mmHg, pulse is 95/min, respirations are 22/min. He states that his blood pressure usually runs low. His physical exam is notable for an unremarkable cardiac exam, bibasilar crackles, and RLQ tenderness with rebound tenderness when the LLQ is palpated. Laboratory results are shown below: Hemoglobin: 11 g/dL Hematocrit: 35 % Leukocyte count: 16,000/mm^3 with normal differential Platelet count: 190,000/mm^3 Serum: Na+: 137 mEq/L Cl-: 100 mEq/L K+: 3.7 mEq/L HCO3-: 23 mEq/L BUN: 40 mg/dL Glucose: 110 mg/dL Creatinine: 0.8 mg/dL Ca2+: 9.1 mg/dL AST: 34 U/L ALT: 45 U/L International normalized ratio (INR): 6.2 Prothrombin time (PT): 40 seconds Partial thromboplastin time: 70 seconds Blood type: O Rhesus: Positive Antibody screen: Negative A clinical diagnosis is made and supported by the surgical consult team in lieu of imaging. The next operating room for an add-on procedure will not be available for another 5 hours. Appropriate medical therapy is initiated. What is the best next step for surgical optimization?
A 77-year-old man with a history of hypertension and a 46 pack-year smoking history presents to the emergency department from an extended care facility with acute onset of headache, nausea, vomiting, and neck pain which started 6 hours ago and has persisted since. He is alert, but his baseline level of consciousness is slightly diminished per the nursing home staff. His temperature is 99.0°F (37.2°C), blood pressure is 164/94 mmHg, pulse is 90/min, respirations are 16/min, and oxygen saturation is 98% on room air. The patient's neurological exam is unremarkable with cranial nerves II-XII grossly intact and with stable gait with a walker. He is immediately sent for a head CT which is normal. What is the most appropriate next step in management?
A 65-year-old man presents to the emergency department for sudden weakness. He was doing mechanical work on his car where he acutely developed right-leg weakness and fell to the ground. He is accompanied by his wife, who said that this has never happened before. He was last seen neurologically normal approximately 2 hours prior to presentation. His past medical history is significant for hypertension and type II diabetes. His temperature is 98.8°F (37.1°C), blood pressure is 177/108 mmHg, pulse is 90/min, respirations are 15/min, and oxygen saturation is 99% on room air. Neurological exam reveals that he is having trouble speaking and has profound weakness of his right upper and lower extremity. Which of the following is the best next step in management?
A 77-year-old man is brought to the emergency department by his wife because of headache, nausea, and vomiting for 24 hours. His wife says that over the past 2 weeks, he has been more irritable and has had trouble remembering to do routine errands. Two weeks ago, he fell during a skiing accident but did not lose consciousness. He has coronary artery disease and hypertension. He has smoked one pack of cigarettes daily for 50 years. He has had 2 glasses of wine daily since his retirement 10 years ago. Current medications include atenolol, enalapril, furosemide, atorvastatin, and aspirin. He appears acutely ill. He is oriented to person but not to place or time. His temperature is 37°C (98.6°F), pulse is 99/min, respirations are 16/min, and blood pressure is 160/90 mm Hg. During the examination, he is uncooperative and unable to answer questions. Deep tendon reflexes are 4+ on the left and 2+ on the right. Babinski's sign is present on the left. There is mild weakness of the left iliopsoas and hamstring muscles. A CT scan of the head without contrast shows a high-density, 15-mm crescentic collection across the right hemispheric convexity. Which of the following is the most appropriate next step in the management of this patient?
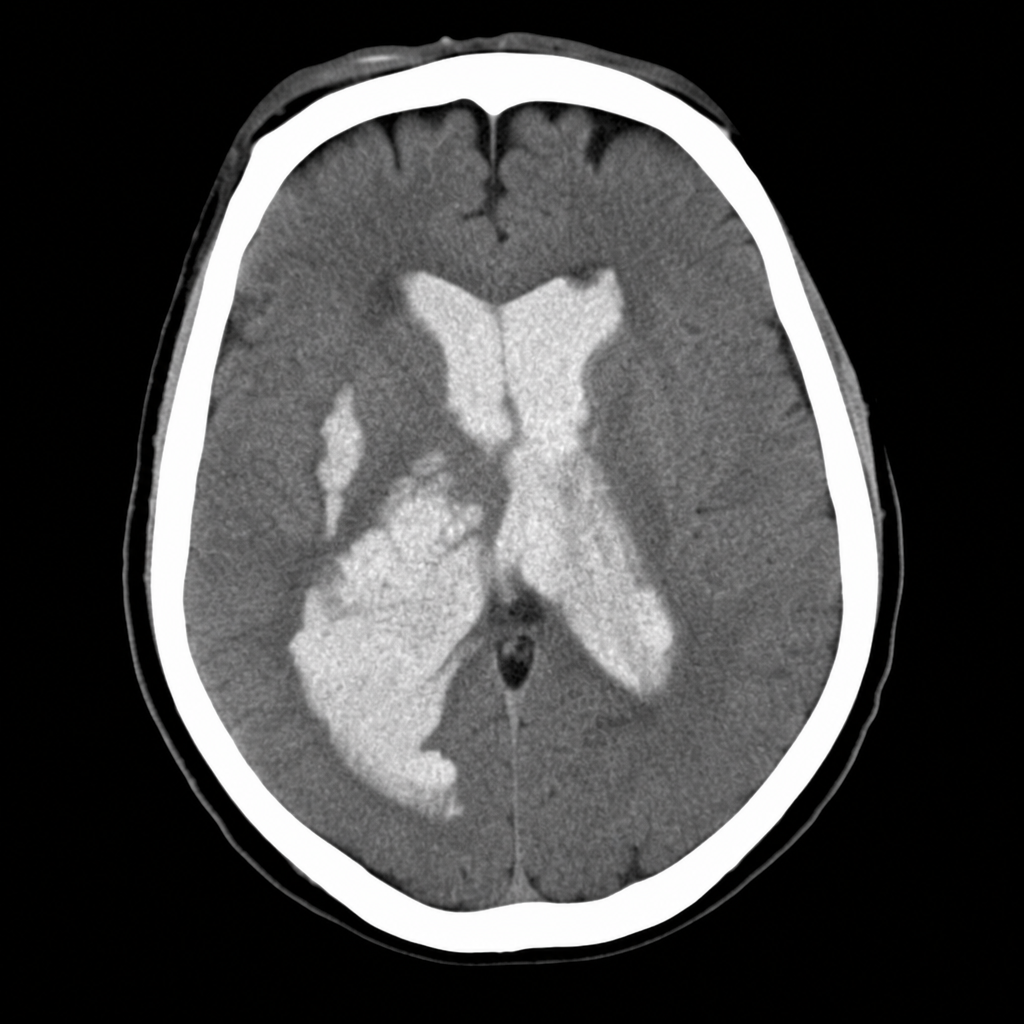
A 58-year-old woman is brought to the emergency department after sudden onset of the worst headache of her life followed by loss of consciousness. She is now obtunded with a GCS of 10. Vital signs: BP 192/110 mmHg, HR 96 bpm, SpO2 94% on room air. The emergency physician reviews the CT head image shown. Based on the imaging finding, which of the following is the most appropriate immediate management decision?
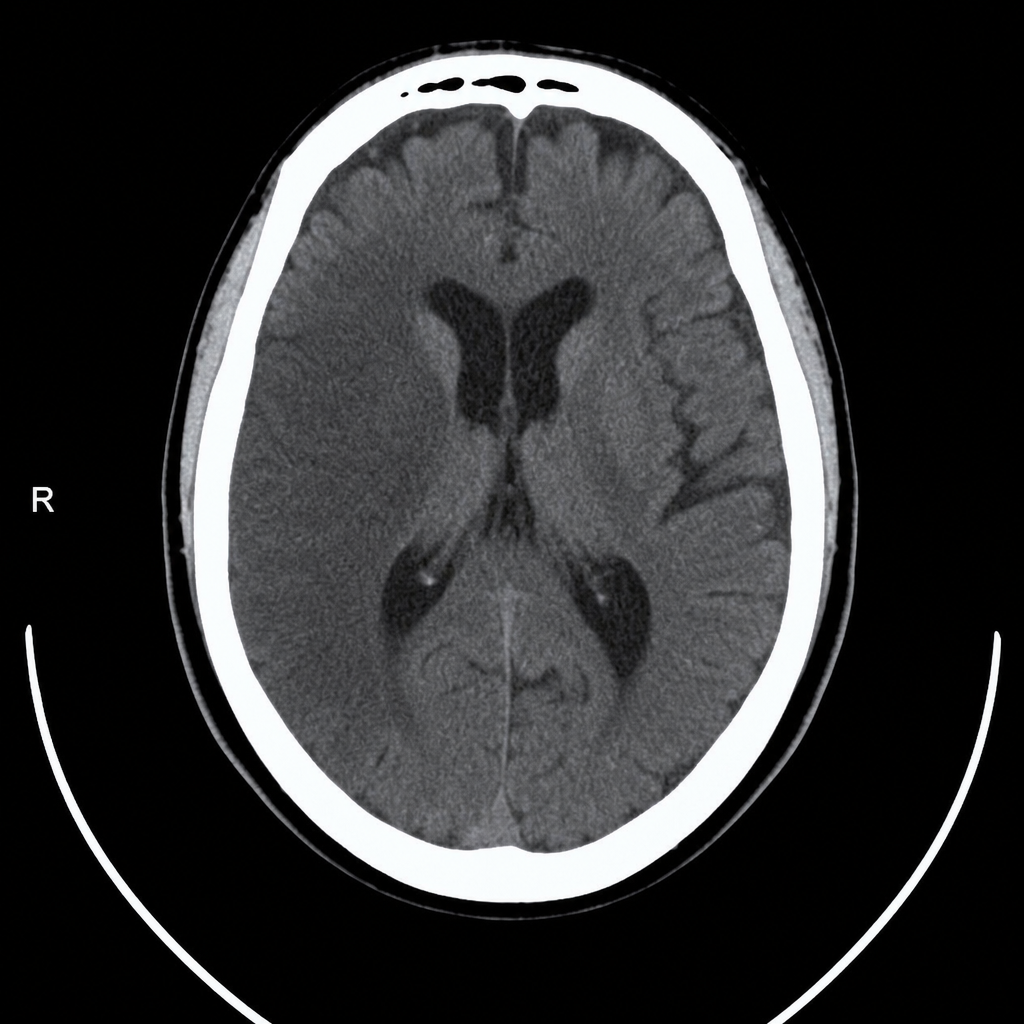
A 67-year-old man with hypertension and type 2 diabetes is brought to the emergency department by his wife, who noticed he was unable to lift his right arm and his speech became slurred 2 hours ago. Vital signs: BP 188/104 mmHg, HR 82 bpm, RR 16, SpO2 97% on room air. Neurological exam reveals right-sided facial droop, right arm weakness (2/5), and dysarthria; NIHSS score is 14. A non-contrast CT head is performed and reviewed. The image is shown above. His blood pressure must be controlled before alteplase can be given. Which of the following is the most appropriate next step in management?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app