
Ischemic vs hemorrhagic stroke differentiation — MCQs

A 48-year-old man presents to the ER with a sudden-onset, severe headache. He is vomiting and appears confused. His wife, who accompanied him, says that he has not had any trauma, and that the patient has no relevant family history. He undergoes a non-contrast head CT that shows blood between the arachnoid and pia mater. What is the most likely complication from this condition?
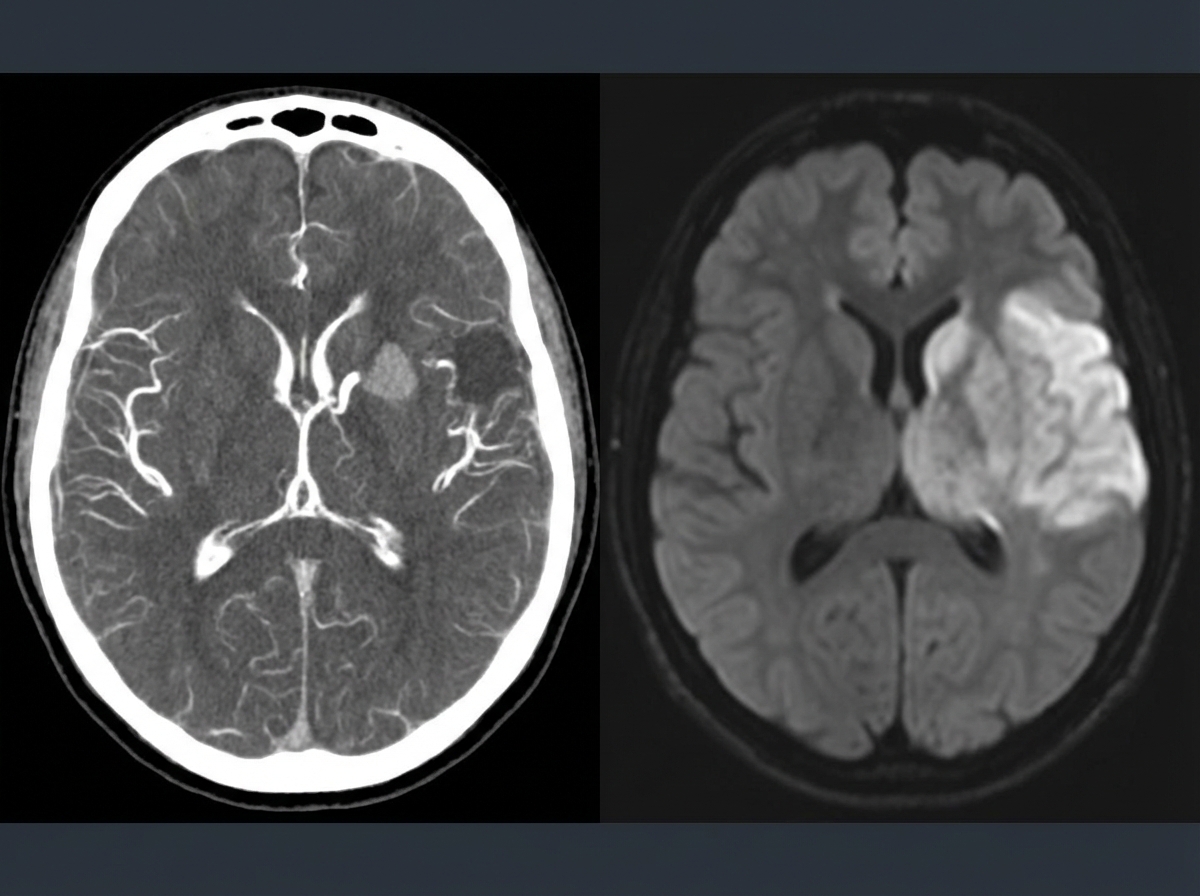
A 69-year-old man is brought in by his wife with acute onset aphasia for the past 5 hours. The patient's wife says that they were sitting having dinner when suddenly he was not able to speak. They delayed coming to the hospital because he had a similar episode 2 months ago which resolved within an hour. His past medical history is significant for hypercholesterolemia, managed with rosuvastatin, and a myocardial infarction (MI) 2 months ago, status post percutaneous transluminal coronary angioplasty complicated by residual angina. His family history is significant for his father who died of MI at age 60. The patient reports a 15-pack-year smoking history but denies any alcohol or recreational drug use. The vital signs include: temperature 37.0℃ (98.6℉), blood pressure 125/85 mm Hg, pulse 96/min, and respiratory rate 19/min. On physical examination, the patient has expressive aphasia. There is a weakness of the right-sided lower facial muscles. The strength in his upper and lower extremities is 4/5 on the right and 5/5 on the left. There is also a decreased sensation on his right side. A noncontrast computed tomography (CT) scan of the head is unremarkable. CT angiography (CTA) and diffusion-weighted magnetic resonance imaging (MRI) of the brain are acquired, and the findings are shown in the exhibit (see image). Which of the following is the best course of treatment in this patient?
A 60-year-old male is admitted to the ICU for severe hypertension complicated by a headache. The patient has a past medical history of insulin-controlled diabetes, hypertension, and hyperlipidemia. He smokes 2 packs of cigarettes per day. He states that he forgot to take his medications yesterday and started getting a headache about one hour ago. His vitals on admission are the following: blood pressure of 160/110 mmHg, pulse 95/min, temperature 98.6 deg F (37.2 deg C), and respirations 20/min. On exam, the patient has an audible abdominal bruit. After administration of antihypertensive medications, the patient has a blood pressure of 178/120 mmHg. The patient reports his headache has increased to a 10/10 pain level, that he has trouble seeing, and he can't move his extremities. After stabilizing the patient, what is the best next step to diagnose the patient's condition?
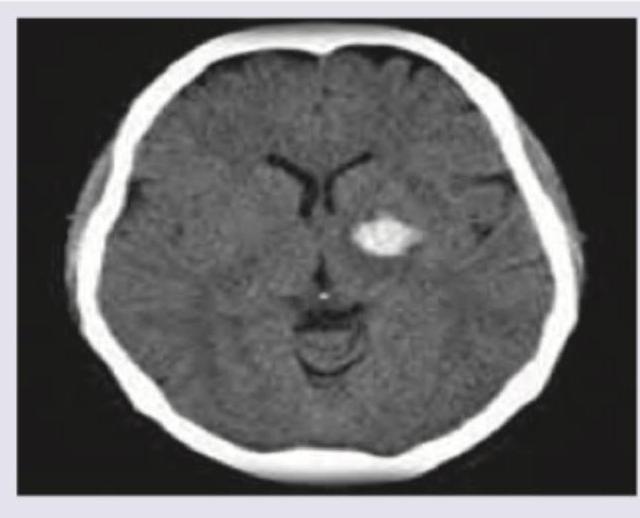
A 53-year-old man is brought to the emergency department for confusion. He was in his usual state of health until about 3 hours ago when he tried to use his sandwich to turn off the TV. He also complained to his wife that he had a severe headache. Past medical history is notable for hypertension, which has been difficult to control on multiple medications. His temperature is 36.7°C (98°F), the pulse is 70/min, and the blood pressure is 206/132 mm Hg. On physical exam he is alert and oriented only to himself, repeating over and over that his head hurts. The physical exam is otherwise unremarkable and his neurologic exam is nonfocal. The noncontrast CT scan of the patient's head is shown and reveals an acute intraparenchymal hemorrhage in the basal ganglia. Which of the following diagnostic tests would be most helpful in determining the underlying cause of this patient's hemorrhage?
A 73-year-old man is brought to the emergency department by ambulance after being found to be non-communicative by his family during dinner. On presentation he appears to be alert, though he is confused and cannot follow instructions. When he tries to speak, he vocalizes a string of fluent but unintelligible syllables. Given this presentation, his physician decides to administer tissue plasminogen activator to this patient. This intervention best represents which of the following principles?
A 75-year-old woman presents with sudden loss of vision. She says that she was reading when suddenly she was not able to see the print on half of the page. Her symptoms started 4 hours ago and are accompanied by a severe posterior headache. Vital signs reveal the following: blood pressure 119/76 mm Hg, pulse 89/min, SpO2 98% on room air. The patient was unable to recognize her niece when she arrived to see her. A noncontrast CT of the head shows no evidence of hemorrhagic stroke. What is the most likely diagnosis in this patient?
A 72-year-old man is brought into clinic by his daughter for increasing confusion. The daughter states that over the past 2 weeks, she has noticed that the patient “seems to stare off into space.” She reports he has multiple episodes a day during which he will walk into a room and forget why. She is also worried about his balance. She endorses that he has had several falls, the worst being 3 weeks ago when he tripped on the sidewalk getting the mail. The patient denies loss of consciousness, pre-syncope, chest pain, palpitations, urinary incontinence, or bowel incontinence. He complains of headache but denies dizziness. He reports nausea and a few episodes of non-bloody emesis but denies abdominal pain, constipation, or diarrhea. The patient’s medical history is significant for atrial fibrillation, diabetes, hypertension, hyperlipidemia, and osteoarthritis. He takes aspirin, warfarin, insulin, lisinopril, simvastatin, and ibuprofen. He drinks a half glass of whisky after dinner every night and smokes a cigar on the weekends. On physical examination, he is oriented to name and place but not to date. He is unable to spell "world" backward. When asked to remember 3 words, he recalls only 2. There are no motor or sensory deficits. Which of the following is the most likely diagnosis?
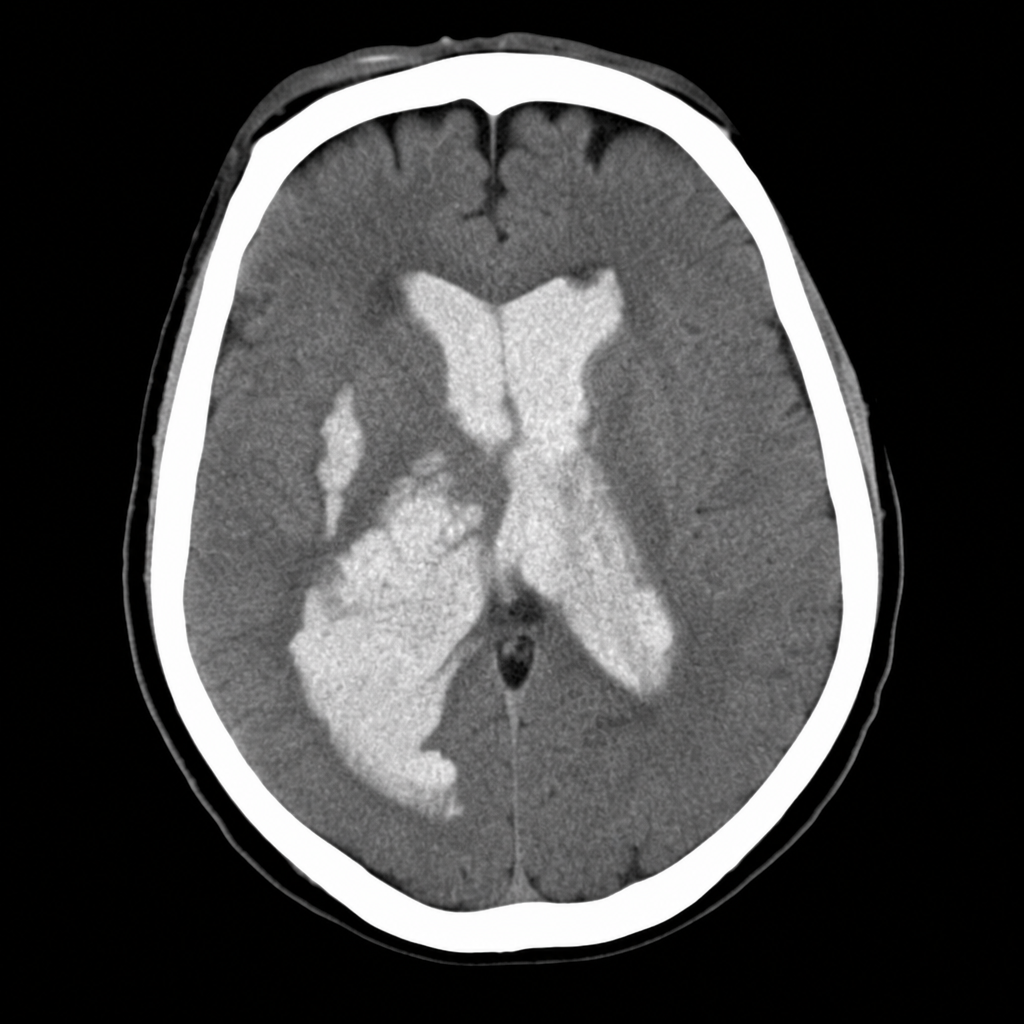
A 58-year-old woman is brought to the emergency department after sudden onset of the worst headache of her life followed by loss of consciousness. She is now obtunded with a GCS of 10. Vital signs: BP 192/110 mmHg, HR 96 bpm, SpO2 94% on room air. The emergency physician reviews the CT head image shown. Based on the imaging finding, which of the following is the most appropriate immediate management decision?
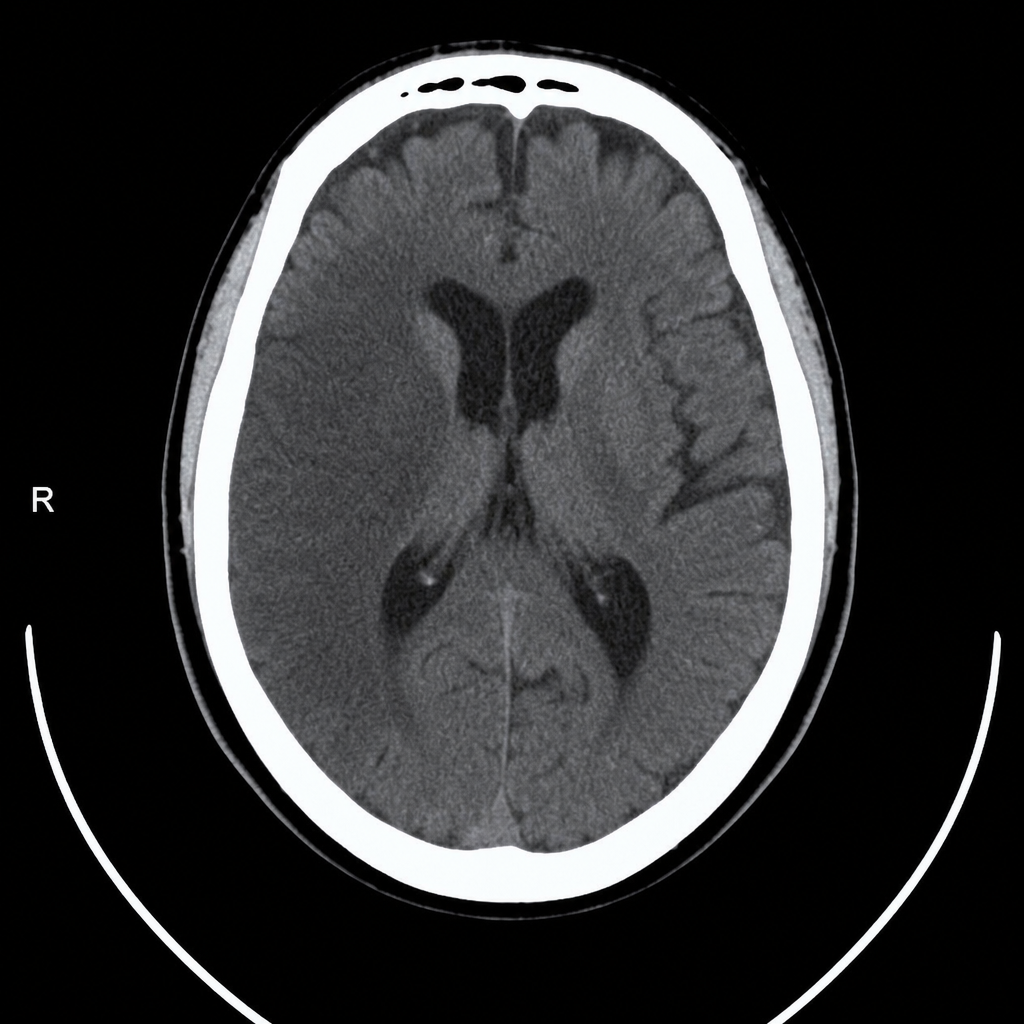
A 67-year-old man with hypertension and type 2 diabetes is brought to the emergency department by his wife, who noticed he was unable to lift his right arm and his speech became slurred 2 hours ago. Vital signs: BP 188/104 mmHg, HR 82 bpm, RR 16, SpO2 97% on room air. Neurological exam reveals right-sided facial droop, right arm weakness (2/5), and dysarthria; NIHSS score is 14. A non-contrast CT head is performed and reviewed. The image is shown above. His blood pressure must be controlled before alteplase can be given. Which of the following is the most appropriate next step in management?
A 48-year-old woman presents with acute stroke symptoms 18 hours ago. MRI shows a right MCA M1 occlusion with large penumbra on perfusion imaging (mismatch ratio >1.8) and small infarct core (25 mL). Her NIHSS is 16. She has no significant comorbidities. Her family is concerned about disability but wants to pursue treatment if reasonable chance of benefit exists. Synthesize the evidence and evaluate the treatment approach.
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app