
Acute ischemic stroke management — MCQs

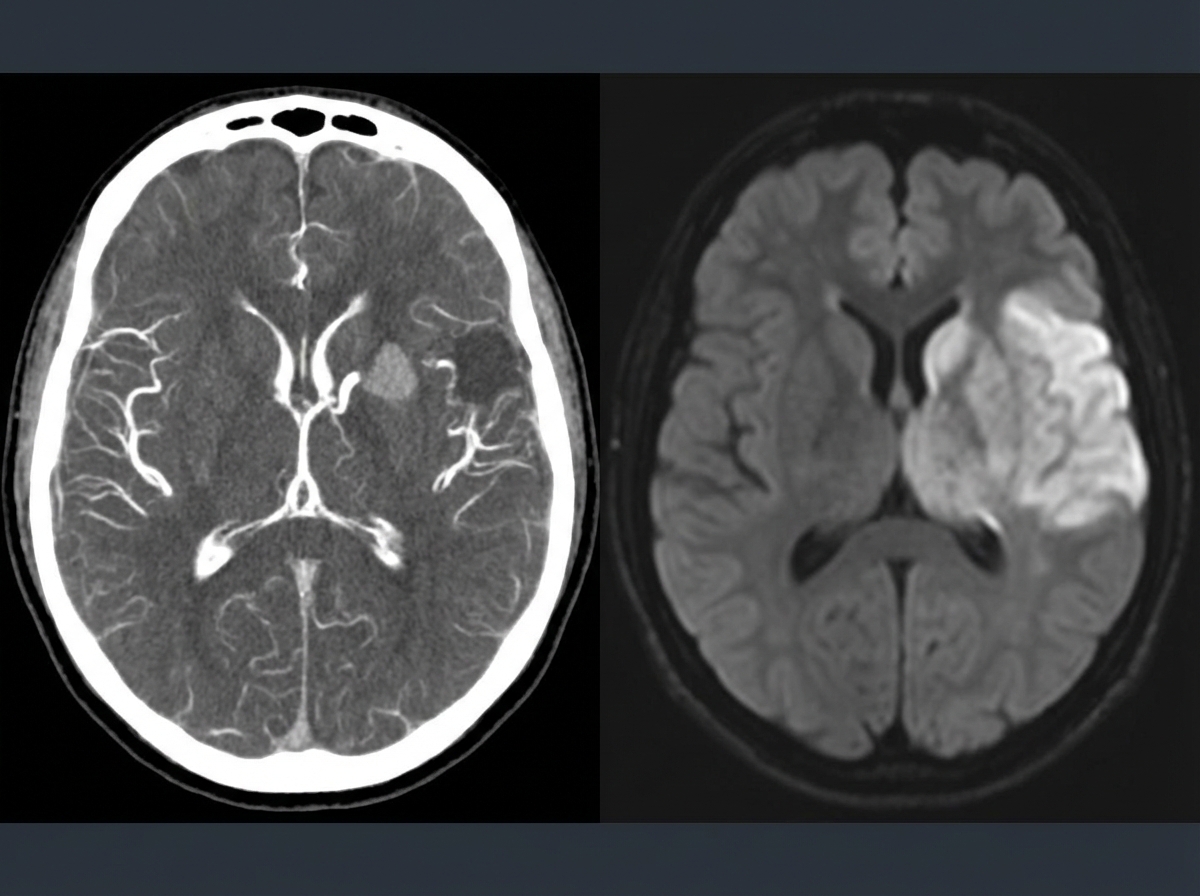
A 69-year-old man is brought in by his wife with acute onset aphasia for the past 5 hours. The patient's wife says that they were sitting having dinner when suddenly he was not able to speak. They delayed coming to the hospital because he had a similar episode 2 months ago which resolved within an hour. His past medical history is significant for hypercholesterolemia, managed with rosuvastatin, and a myocardial infarction (MI) 2 months ago, status post percutaneous transluminal coronary angioplasty complicated by residual angina. His family history is significant for his father who died of MI at age 60. The patient reports a 15-pack-year smoking history but denies any alcohol or recreational drug use. The vital signs include: temperature 37.0℃ (98.6℉), blood pressure 125/85 mm Hg, pulse 96/min, and respiratory rate 19/min. On physical examination, the patient has expressive aphasia. There is a weakness of the right-sided lower facial muscles. The strength in his upper and lower extremities is 4/5 on the right and 5/5 on the left. There is also a decreased sensation on his right side. A noncontrast computed tomography (CT) scan of the head is unremarkable. CT angiography (CTA) and diffusion-weighted magnetic resonance imaging (MRI) of the brain are acquired, and the findings are shown in the exhibit (see image). Which of the following is the best course of treatment in this patient?
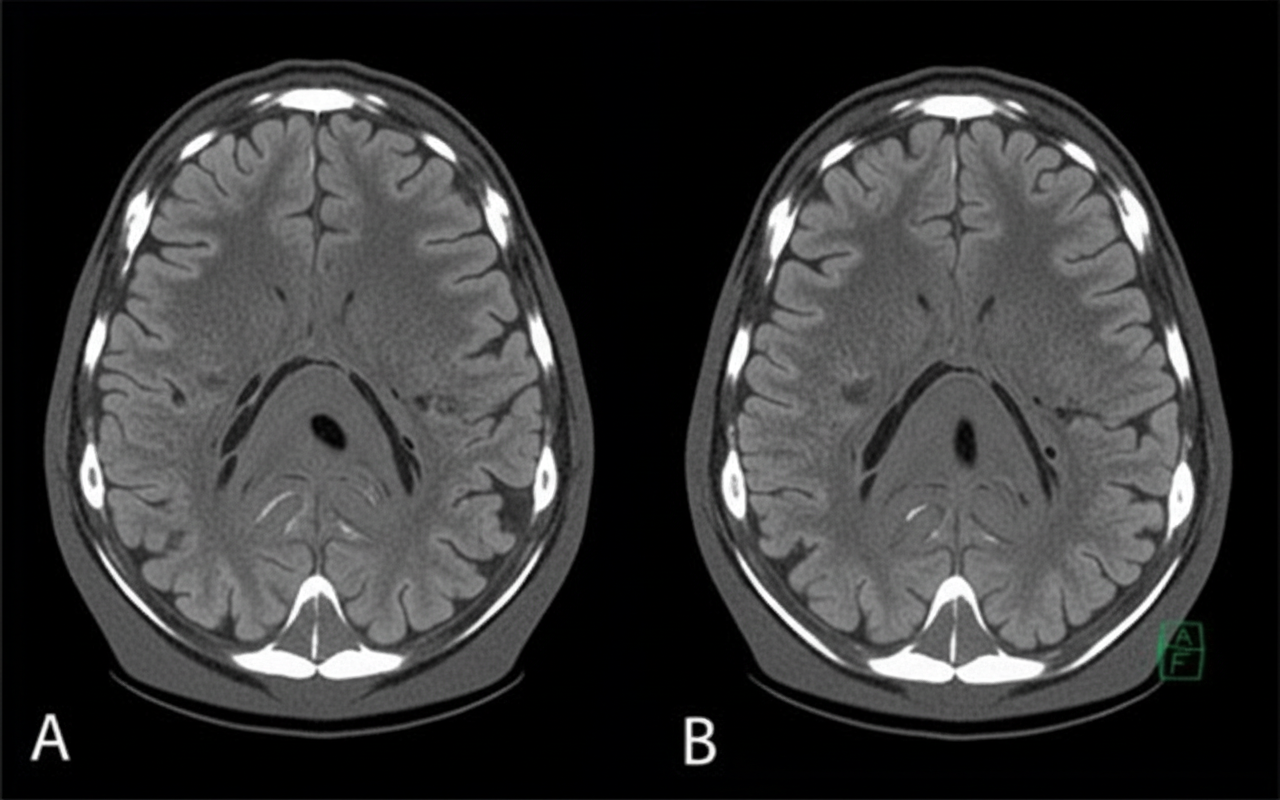
A 58-year-old man presents to the clinic concerned about his health after his elder brother recently became bed-bound due to a brain condition. He has also brought a head CT scan of his brother to reference, as shown in the picture. The patient has type 2 diabetes mellitus, hypertension, osteoarthritis, and hypercholesterolemia. His medication list includes aspirin, diclofenac sodium, metformin, and ramipril. He leads a sedentary lifestyle and smokes one pack of cigarettes daily. He also drinks 4–5 cups of red wine every weekend. His BMI is 33.2 kg/m2. His blood pressure is 164/96 mm Hg, the heart rate is 84/min, and the respiratory rate is 16/min. Which of the following interventions will be most beneficial for reducing the risk of developing the disease that his brother has?
A 79-year-old man is brought to the emergency department after he noted the abrupt onset of weakness accompanied by decreased sensation on his left side. His symptoms developed rapidly, peaked within 1 minute, and began to spontaneously resolve 10 minutes later. Upon arrival in the emergency room 40 minutes after the initial onset of symptoms, they had largely resolved. The patient has essential hypertension, type 2 diabetes mellitus, chronic obstructive pulmonary disease, and a 50 pack-year smoking history. He also had an ST-elevation myocardial infarction 3 years ago. His brain CT scan without contrast is reported as normal. Carotid duplex ultrasonography reveals 90% stenosis of the right internal carotid. His transthoracic echocardiogram does not reveal any intracardiac abnormalities. Which of the following interventions is most appropriate for this patient's condition?
A 74-year-old man is rushed to the emergency department with left-sided weakness, facial deviation, and slurred speech. His wife first noticed these changes about an hour ago. The patient is having difficulty communicating. He can answer questions by nodding his head, and his wife is providing detailed information. He denies fever, loss of consciousness, head injury, bleeding, or seizures. Past medical history is significant for diabetes mellitus, hypertension, hyperlipidemia, ischemic heart disease, chronic kidney disease, and osteoarthritis. He had a heart attack 6 weeks ago. Baseline creatinine is 2.5 mg/dL, and he is not on hemodialysis. Medications include aspirin, clopidogrel, metoprolol, ramipril, rosuvastatin, and insulin detemir. Blood pressure is 175/95 mm Hg and the heart rate is 121/min. Muscle strength is decreased in both the upper and lower extremities on the left-side. A forehead sparing left sided facial weakness is also appreciated. An ECG reveals atrial fibrillation. An urgent head CT shows a hypodense area in the right parietal cortex with no indication of hemorrhage. Treatment with tissue plasminogen activator (tPA) is deferred due to which condition?
A 69-year-old male presents to the emergency department for slurred speech and an inability to use his right arm which occurred while he was eating dinner. The patient arrived at the emergency department within one hour. A CT scan was performed of the head and did not reveal any signs of hemorrhage. The patient is given thrombolytics and is then managed on the neurology floor. Three days later, the patient is recovering and is stable. He seems depressed but is doing well with his symptoms gradually improving as compared to his initial presentation. The patient complains of neck pain that has worsened slowly over the past few days for which he is being given ibuprofen. Laboratory values are ordered and return as indicated below: Serum: Na+: 130 mEq/L K+: 3.7 mEq/L Cl-: 100 mEq/L HCO3-: 24 mEq/L Urea nitrogen: 7 mg/dL Glucose: 70 mg/dL Creatinine: 0.9 mg/dL Ca2+: 9.7 mg/dL Urine: Appearance: dark Glucose: negative WBC: 0/hpf Bacterial: none Na+: 320 mEq/L/24 hours His temperature is 99.5°F (37.5°C), pulse is 95/min, blood pressure is 129/70 mmHg, respirations are 10/min, and oxygen saturation is 98% on room air. Which of the following is the best next step in management?
A 77-year-old woman is brought by ambulance to the emergency department after she developed weakness of her right arm along with a right-sided facial droop. By the time the ambulance arrived, she was having difficulty speaking. Past medical history is significant for hypertension, diabetes mellitus type II, and hyperlipidemia. She takes lisinopril, hydrochlorothiazide, metformin, and atorvastatin. On arrival to the emergency department, her vital signs are within normal limits. On physical examination, she is awake and alert but the right side of her mouth is dropping, making it difficult for her to speak clearly. Her heart has a regular rate and rhythm and her lungs are clear to auscultation bilaterally. Fingerstick glucose is 85 mg/dL. Her right upper extremity strength is 2/5 and her left upper extremity strength is 5/5. Which of the following is the best next step in management?
A 73-year-old man is brought to the emergency department by ambulance after being found to be non-communicative by his family during dinner. On presentation he appears to be alert, though he is confused and cannot follow instructions. When he tries to speak, he vocalizes a string of fluent but unintelligible syllables. Given this presentation, his physician decides to administer tissue plasminogen activator to this patient. This intervention best represents which of the following principles?
A 77-year-old man with a history of hypertension and a 46 pack-year smoking history presents to the emergency department from an extended care facility with acute onset of headache, nausea, vomiting, and neck pain which started 6 hours ago and has persisted since. He is alert, but his baseline level of consciousness is slightly diminished per the nursing home staff. His temperature is 99.0°F (37.2°C), blood pressure is 164/94 mmHg, pulse is 90/min, respirations are 16/min, and oxygen saturation is 98% on room air. The patient's neurological exam is unremarkable with cranial nerves II-XII grossly intact and with stable gait with a walker. He is immediately sent for a head CT which is normal. What is the most appropriate next step in management?
A 72-year-old man is brought into clinic by his daughter for increasing confusion. The daughter states that over the past 2 weeks, she has noticed that the patient “seems to stare off into space.” She reports he has multiple episodes a day during which he will walk into a room and forget why. She is also worried about his balance. She endorses that he has had several falls, the worst being 3 weeks ago when he tripped on the sidewalk getting the mail. The patient denies loss of consciousness, pre-syncope, chest pain, palpitations, urinary incontinence, or bowel incontinence. He complains of headache but denies dizziness. He reports nausea and a few episodes of non-bloody emesis but denies abdominal pain, constipation, or diarrhea. The patient’s medical history is significant for atrial fibrillation, diabetes, hypertension, hyperlipidemia, and osteoarthritis. He takes aspirin, warfarin, insulin, lisinopril, simvastatin, and ibuprofen. He drinks a half glass of whisky after dinner every night and smokes a cigar on the weekends. On physical examination, he is oriented to name and place but not to date. He is unable to spell "world" backward. When asked to remember 3 words, he recalls only 2. There are no motor or sensory deficits. Which of the following is the most likely diagnosis?
A 27-year-old man presents to the emergency department with dizziness. He states he has experienced a sustained sensation of the room spinning that is low grade and constant since this morning. The patient occasionally feels nauseous and has been taking diphenydramine to sleep which helps with his symptoms. The patient is generally healthy, has no other medical conditions, and only endorses eating more garlic recently to get over a cold he had a few days ago. His temperature is 98.7°F (37.1°C), blood pressure is 122/81 mmHg, pulse is 82/min, respirations are 15/min, and oxygen saturation is 99% on room air. Physical exam is notable for a healthy man. The patient is sat upright, his head is turned slightly to the right, and he is laid back flat rapidly. This does not provoke any symptoms even when repeated on the left side. A nystagmus is notable on cranial nerve exam as well as bilateral decreased hearing. The patient’s tandem gait is unstable; however, his baseline gait appears unremarkable despite the patient stating he has a sustained sensation of imbalance. Which of the following is the most likely diagnosis?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app