
Stroke — MCQs

On this page
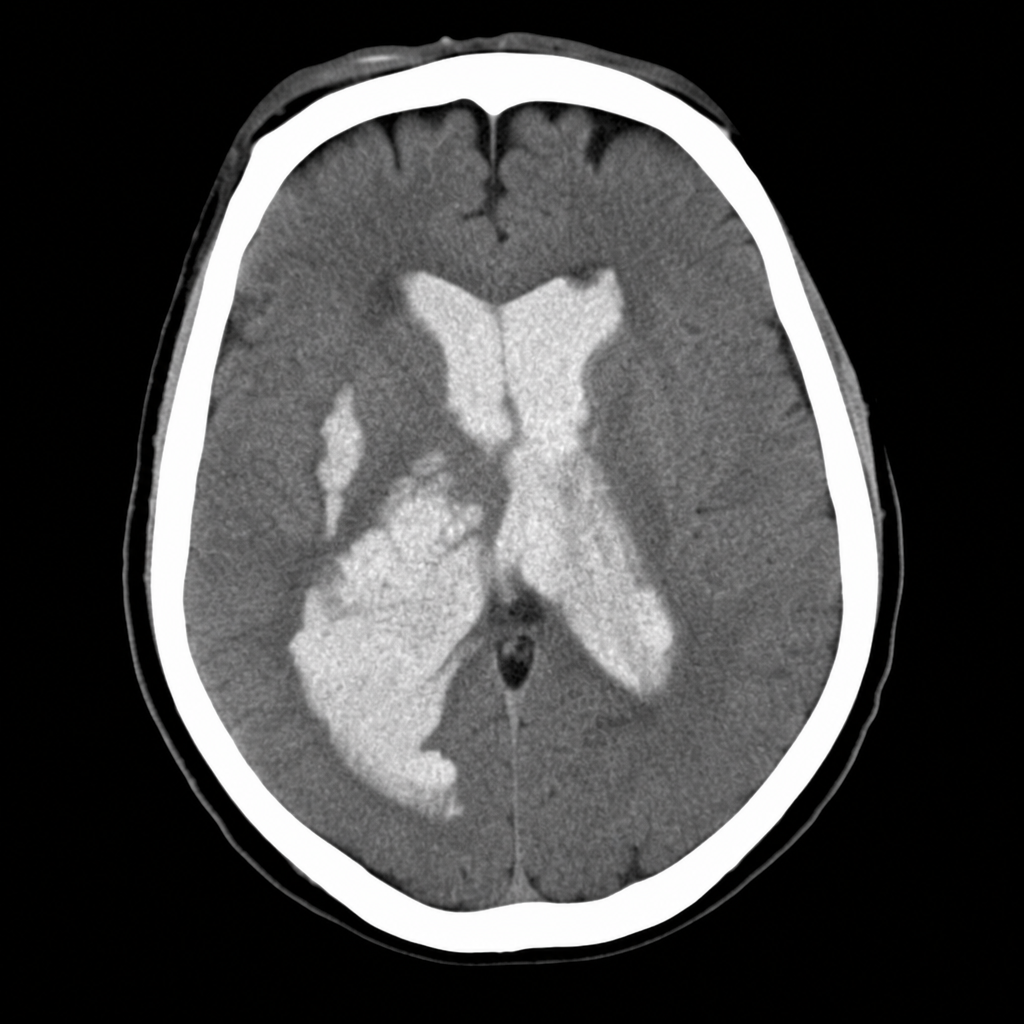
A 58-year-old woman is brought to the emergency department after sudden onset of the worst headache of her life followed by loss of consciousness. She is now obtunded with a GCS of 10. Vital signs: BP 192/110 mmHg, HR 96 bpm, SpO2 94% on room air. The emergency physician reviews the CT head image shown. Based on the imaging finding, which of the following is the most appropriate immediate management decision?
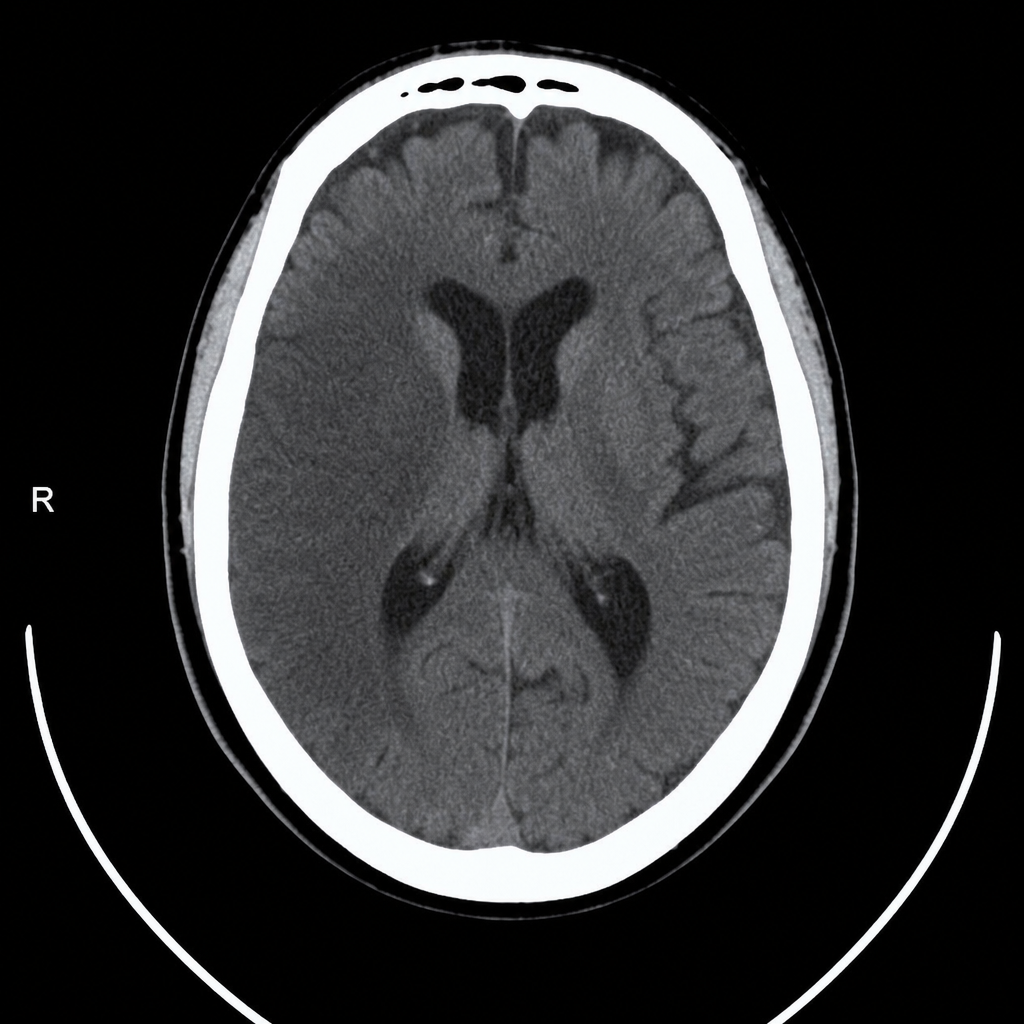
A 67-year-old man with hypertension and type 2 diabetes is brought to the emergency department by his wife, who noticed he was unable to lift his right arm and his speech became slurred 2 hours ago. Vital signs: BP 188/104 mmHg, HR 82 bpm, RR 16, SpO2 97% on room air. Neurological exam reveals right-sided facial droop, right arm weakness (2/5), and dysarthria; NIHSS score is 14. A non-contrast CT head is performed and reviewed. The image is shown above. His blood pressure must be controlled before alteplase can be given. Which of the following is the most appropriate next step in management?
A 48-year-old woman presents with acute stroke symptoms 18 hours ago. MRI shows a right MCA M1 occlusion with large penumbra on perfusion imaging (mismatch ratio >1.8) and small infarct core (25 mL). Her NIHSS is 16. She has no significant comorbidities. Her family is concerned about disability but wants to pursue treatment if reasonable chance of benefit exists. Synthesize the evidence and evaluate the treatment approach.
A 55-year-old man undergoes successful thrombectomy for left MCA occlusion. Post-procedure, he develops progressive lethargy and his blood pressure increases to 180/100 mmHg. CT shows hyperdensity in the treated territory without hemorrhage, and his symptoms worsen over 4 hours despite blood pressure control. Evaluate the most likely diagnosis and management priority.
An 80-year-old woman with atrial fibrillation presents 2 hours after acute ischemic stroke. NIHSS is 22. Imaging shows large left MCA territory infarction involving >1/3 of MCA territory with basilar artery occlusion. She lives alone but was independent before this event. Her family requests all possible interventions. Evaluate the management approach considering benefits versus risks.
Practice by Chapter
Stroke recognition and initial assessment
Practice Questions
Ischemic vs hemorrhagic stroke differentiation
Practice Questions
Acute ischemic stroke management
Practice Questions
Thrombolysis inclusion/exclusion criteria
Practice Questions
Mechanical thrombectomy indications
Practice Questions
Hemorrhagic stroke management
Practice Questions
Blood pressure management in stroke
Practice Questions
Stroke unit care principles
Practice Questions
Swallowing assessment and management
Practice Questions
Secondary stroke prevention
Practice Questions
Rehabilitation principles
Practice Questions
Management of stroke complications
Practice Questions
TIA management and ABCD2 score
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app