
Source identification and control — MCQs

A 35-year-old woman with a medical history significant for asthma, hypertension, and occasional IV drug use comes to the emergency department with fever. On physical exam, there are findings depicted in figure A, for which the patient cannot account. What test will be most helpful to establish the diagnosis?

A 72-year-old female presents to the emergency department complaining of severe abdominal pain and several days of bloody diarrhea. Her symptoms began with intermittent bloody diarrhea five days ago and have worsened steadily. For the last 24 hours, she has complained of fevers, chills, and abdominal pain. She has a history of ulcerative colitis, idiopathic hypertension, and hypothyroidism. Her medications include hydrochlorothiazide, levothyroxine, and sulfasalazine. In the ED, her temperature is 39.1°C (102.4°F), pulse is 120/min, blood pressure is 90/60 mmHg, and respirations are 20/min. On exam, the patient is alert and oriented to person and place, but does not know the day. Her mucus membranes are dry. Heart and lung exam are not revealing. Her abdomen is distended with marked rebound tenderness. Bowel sounds are hyperactive. Serum: Na+: 142 mEq/L Cl-: 107 mEq/L K+: 3.3 mEq/L HCO3-: 20 mEq/L BUN: 15 mg/dL Glucose: 92 mg/dL Creatinine: 1.2 mg/dL Calcium: 10.1 mg/dL Hemoglobin: 11.2 g/dL Hematocrit: 30% Leukocyte count: 14,600/mm^3 with normal differential Platelet count: 405,000/mm^3 What is the next best step in management?
A 17-year-old woman presents to the emergency department with abdominal and pelvic pain. She states it started 3 days ago and it has been getting gradually worse. She states it is diffuse and is located over her abdomen, pelvis, and inside her vagina. She also endorses vaginal pruritus and a discharge from her vagina. The patient works in an ice cream parlor and is sexually active with multiple different partners. Her temperature is 98.0°F (36.7°C), blood pressure is 122/80 mmHg, pulse is 82/min, respirations are 15/min, and oxygen saturation is 98% on room air. Physical exam is notable for a foul smelling vagina with a thin, white discharge. Her abdomen is diffusely tender. The patient is noted to be itching her vagina during the exam. Which of the following is the most appropriate initial step in management?
A 49-year-old woman presents to her physician with a fever accompanied by chills and burning micturition since the past 5 days. She is an otherwise healthy woman with no significant past medical history and has an active sexual life. On physical examination, her temperature is 39.4°C (103.0°F), pulse rate is 90/min, blood pressure is 122/80 mm Hg, and respiratory rate is 14/min. Examination of the abdomen and genitourinary region do not reveal any specific positive findings. The physician orders a urinalysis of fresh unspun urine for this patient which shows 25 WBCs/mL of urine. The physician prescribes an empirical antibiotic and other medications for symptom relief. He also orders a bacteriological culture of her urine. After 48 hours of treatment, the woman returns to the physician to report that her symptoms have not improved. The bacteriological culture report indicates the growth of gram-negative bacilli which are lactose-negative and indole-negative, which produce a substance that hydrolyzes urea to produce ammonia. Which of the following bacteria is the most likely cause of infection in the woman?
A 42-year-old man presents to the emergency department with abdominal pain. The patient was at home watching television when he experienced sudden and severe abdominal pain that prompted him to instantly call emergency medical services. The patient has a past medical history of obesity, smoking, alcoholism, hypertension, and osteoarthritis. His current medications include lisinopril and ibuprofen. His temperature is 98.5°F (36.9°C), blood pressure is 120/97 mmHg, pulse is 130/min, respirations are 22/min, and oxygen saturation is 97% on room air. The patient is in an antalgic position on the stretcher. His abdomen is rigid and demonstrates rebound tenderness and hypoactive bowel sounds. What is the next best step in management?
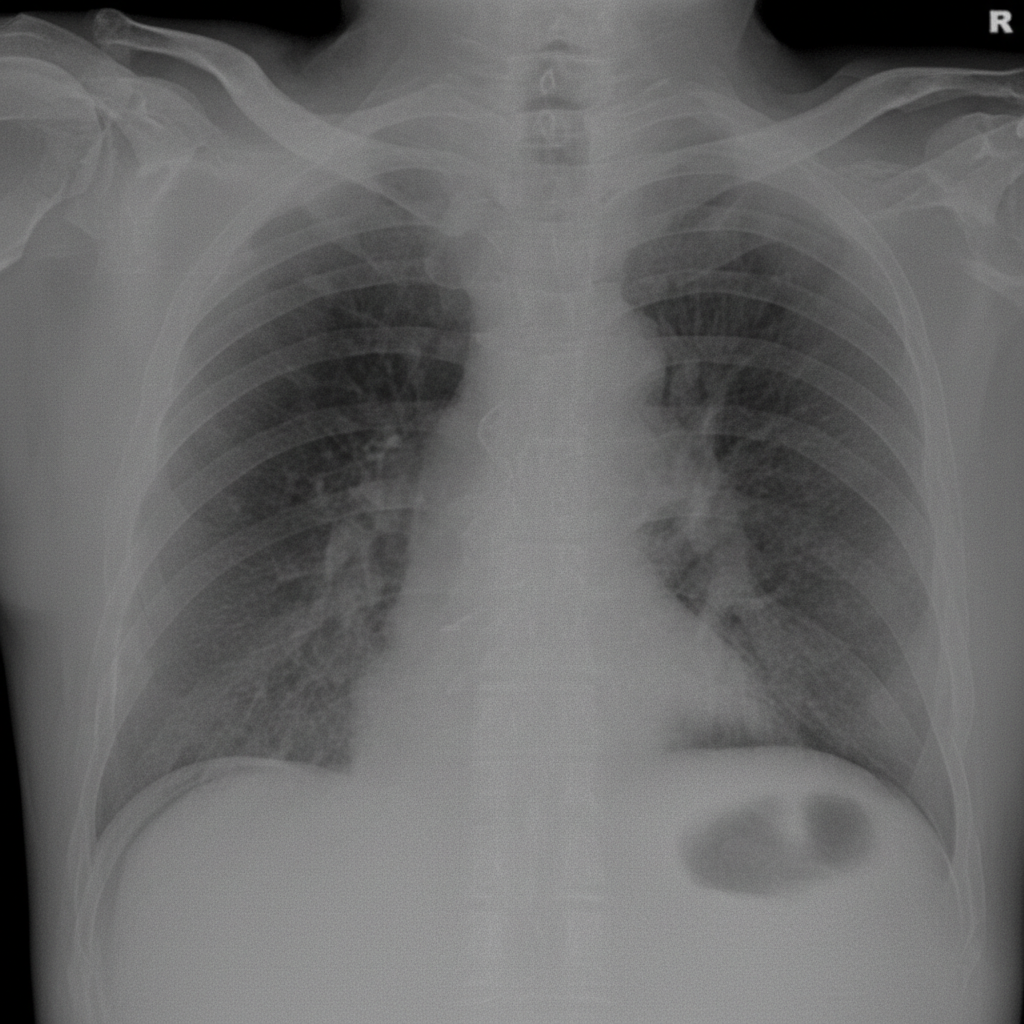
A 56-year-old man is brought to the emergency department after 4 hours of severe abdominal pain with an increase in its intensity over the last hour. His personal history is relevant for peptic ulcer disease and H. pylori infection that is being treated with clarithromycin triple therapy. Upon admission his vital signs are as follows: pulse of 120/min, a respiratory rate of 20/min, body temperature of 39°C (102.2°F), and blood pressure of 90/50 mm Hg. Physical examination reveals significant tenderness over the abdomen. A chest radiograph taken when the patient was standing erect is shown. Which of the following is the next best step in the management of this patient?
A 62-year-old man is brought to the emergency department with fatigue, dry cough, and shortness of breath for 3 days. He reports a slight fever and has also had 3 episodes of watery diarrhea earlier that morning. Last week, he attended a business meeting at a hotel and notes some of his coworkers have also become sick. He has a history of hypertension and hyperlipidemia. He takes atorvastatin, hydrochlorothiazide, and lisinopril. He appears in mild distress. His temperature is 102.1°F (38.9°C), pulse is 56/min, respirations are 16/min, and blood pressure is 150/85 mm Hg. Diffuse crackles are heard in the thorax. Examination shows a soft and nontender abdomen. Laboratory studies show: Hemoglobin 13.5 g/dL Leukocyte count 15,000/mm3 Platelet count 130,000/mm3 Serum Na+ 129 mEq/L Cl- 100 mEq/L K+ 4.6 mEq/L HCO3- 22 mEq/L Urea nitrogen 14 mg/dL Creatinine 1.3 mg/dL An x-ray of the chest shows infiltrates in both lungs. Which of the following is the most appropriate next step in diagnosis?
A 68-year-old man presents to the emergency department with left lower quadrant abdominal pain and fever for 1 day. He states during this time frame he has had weight loss and a decreased appetite. The patient had surgery for a ruptured Achilles tendon 1 month ago and is still recovering but is otherwise generally healthy. His temperature is 102°F (38.9°C), blood pressure is 154/94 mmHg, pulse is 90/min, respirations are 15/min, and oxygen saturation is 98% on room air. Physical exam is remarkable for an uncomfortable and thin man with left lower quadrant abdominal tenderness without rebound findings. Fecal occult test for blood is positive. Laboratory studies are ordered as seen below. Hemoglobin: 10 g/dL Hematocrit: 30% Leukocyte count: 3,500/mm^3 with normal differential Platelet count: 157,000/mm^3 Which of the following is the most appropriate next step in management?
A 55-year-old man, who underwent a kidney transplant 2 years ago, presents in septic shock. He is compliant with his immunosuppressive therapy. He does not use any drugs and is sexually active with one male partner. His complete blood count returns as follows: Hemoglobin: 13.7 g/dL, white blood cell count: 4000 cells/microliter, platelets 250,000 cells/microliter. Of note, from his differential: neutrophils: 10%, lymphocytes: 45%, and monocytes: 7%. His basic metabolic profile is notable for a creatinine remaining at his baseline of 0.9 mg/dL. The patient is started on broad spectrum antibiotics, but his condition does not improve. Fungal blood cultures are obtained and grow Candida species. Which of the following was the most-likely predisposing factor?
A 27-year-old man presents to the emergency department with weakness and a fever for the past week. The patient is homeless and has a past medical history of alcohol and IV drug abuse. His temperature is 102°F (38.9°C), blood pressure is 107/68 mmHg, pulse is 120/min, respirations are 17/min, and oxygen saturation is 98% on room air. Physical exam is notable for a tremulous patient with antecubital scars and a murmur over the left lower sternal border. Blood cultures are drawn and the patient is started on vancomycin and ceftriaxone and is admitted to the ICU. The patient's fever and symptoms do not improve despite antibiotic therapy for which the initial identified organism is susceptible. Cultures currently reveal MRSA as one of the infective organisms. Which of the following is the best next step in management?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app