
Sepsis-induced organ dysfunction management — MCQs

A previously healthy 35-year-old woman is brought into the emergency department after being found unresponsive by her husband. Her husband finds an empty bottle of diazepam tablets in her pocket. She is stuporous. At the hospital, her blood pressure is 90/40 mm Hg, the pulse is 58/min, and the respirations are 6/min. The examination of the pupils shows normal size and reactivity to light. Deep tendon reflexes are 1+ bilaterally. Babinski sign is absent. All 4 extremities are hypotonic. The patient is intubated and taken to the critical care unit for mechanical ventilation and treatment. Regarding the prevention of pneumonia in this patient, which of the following strategies is most likely to achieve this goal?
You are called to a hemodialysis suite. The patient is a 61-year-old man with a history of hypertension, hypercholesterolemia, and type-2 diabetes mellitus-induced end-stage renal disease who has required hemodialysis for the past year. His current hemodialysis session is nearing the end when the nurse notices that his blood pressure has dropped to 88/60 mm Hg from his normal of 142/90 mm Hg. The patient denies any shortness of breath or chest pain. He took his daily bisoprolol, metformin, and insulin this morning before coming to the hospital. On examination, the patient’s blood pressure is 92/60 mm Hg, and his heart rate is 119/min. Chest auscultation is unremarkable. What is the most appropriate next management step?
A 61-year-old female with congestive heart failure and type 2 diabetes is brought to the emergency room by her husband because of an altered mental status. He states he normally helps her be compliant with her medications, but he had been away for several days. On physical exam, her temperature is 37.2 C, BP 85/55, and HR 130. Serum glucose is 500 mg/dL. Which of the following is the first step in the management of this patient?
A 70-year-old man with a recent above-the-knee amputation of the left lower extremity, due to wet gangrene secondary to refractory peripheral artery disease, presents with weakness and dizziness. He says that the symptoms began acutely 24 hours after surgery and have not improved. The amputation was complicated by substantial blood loss. He was placed on empiric antibiotic therapy with ciprofloxacin and clindamycin before the procedure, and blood and wound culture results are still pending. The medical history is significant for type 2 diabetes mellitus and hypertension. Current medications are metformin and lisinopril. The family history is significant for type 2 diabetes mellitus in both parents. Review of symptoms is significant for palpitations and a mild headache for the past 24 hours. His temperature is 38.2°C (100.8°F); blood pressure, 120/70 mm Hg (supine); pulse, 102/min; respiratory rate, 16/min; and oxygen saturation, 99% on room air. When standing, the blood pressure is 90/65 mm Hg and the pulse is 115/min. On physical examination, the patient appears pale and listless. The surgical amputation site does not show any signs of ongoing blood loss or infection. Laboratory tests and an ECG are pending. Which of the following is the next best step in management?
A 14-year-old female with no past medical history presents to the emergency department with nausea and abdominal pain. On physical examination, her blood pressure is 78/65, her respiratory rate is 30, her breath has a fruity odor, and capillary refill is > 3 seconds. Serum glucose is 820 mg/dL. After starting IV fluids, what is the next best step in the management of this patient?
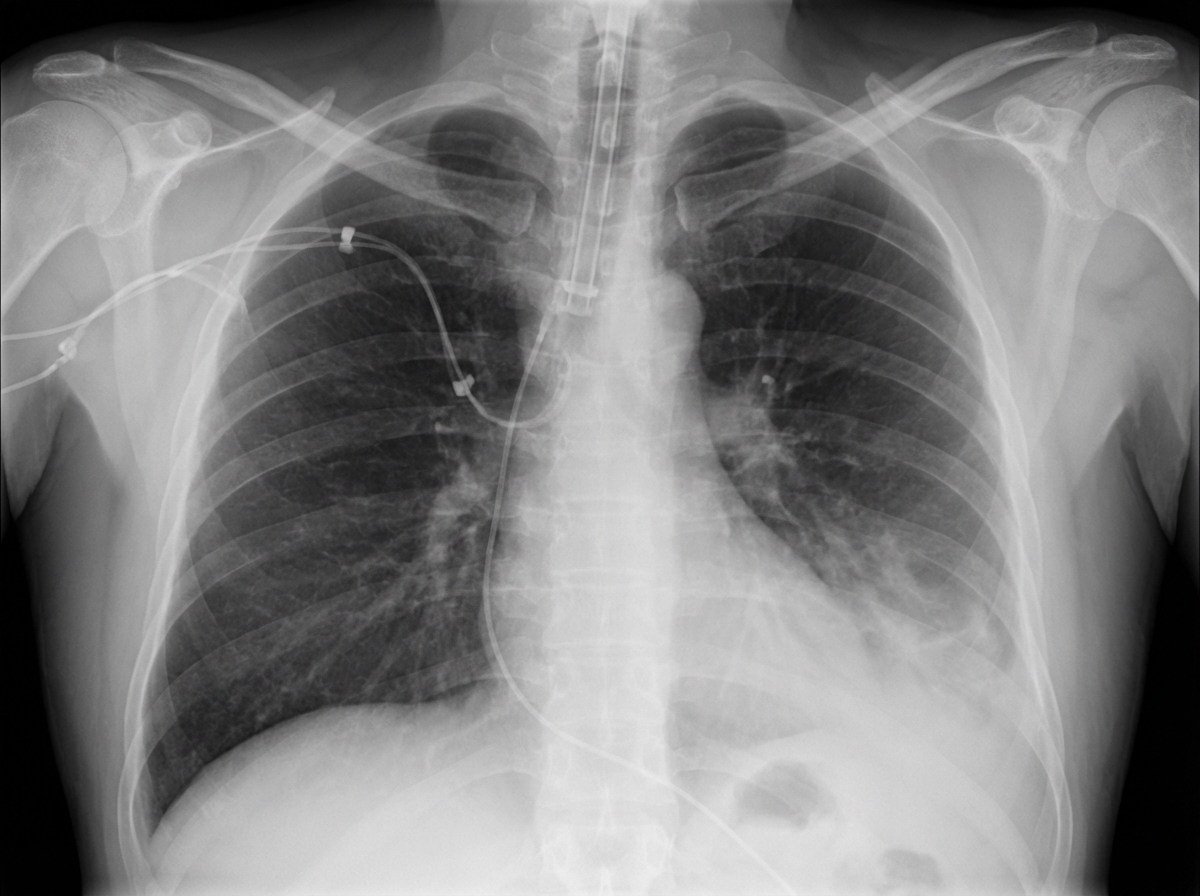
A 63-year-old man is brought to the emergency department, 30 minutes after being involved in a high-speed motor vehicle collision. He is obtunded on arrival. He is intubated and mechanical ventilation is begun. The ventilator is set at a FiO2 of 60%, tidal volume of 440 mL, and positive end-expiratory pressure of 4 cm H2O. On the third day of intubation, his temperature is 37.3°C (99.1°F), pulse is 91/min, and blood pressure is 103/60 mm Hg. There are decreased breath sounds over the left lung base. Cardiac examination shows no abnormalities. The abdomen is soft and not distended. Arterial blood gas analysis shows: pH 7.49 pCO2 29 mm Hg pO2 73 mm Hg HCO3- 20 mEq/L O2 saturation 89% Monitoring shows a sudden increase in the plateau airway pressure. An x-ray of the chest shows deepening of the costophrenic angle on the left side. Which of the following is the most appropriate next step in management?
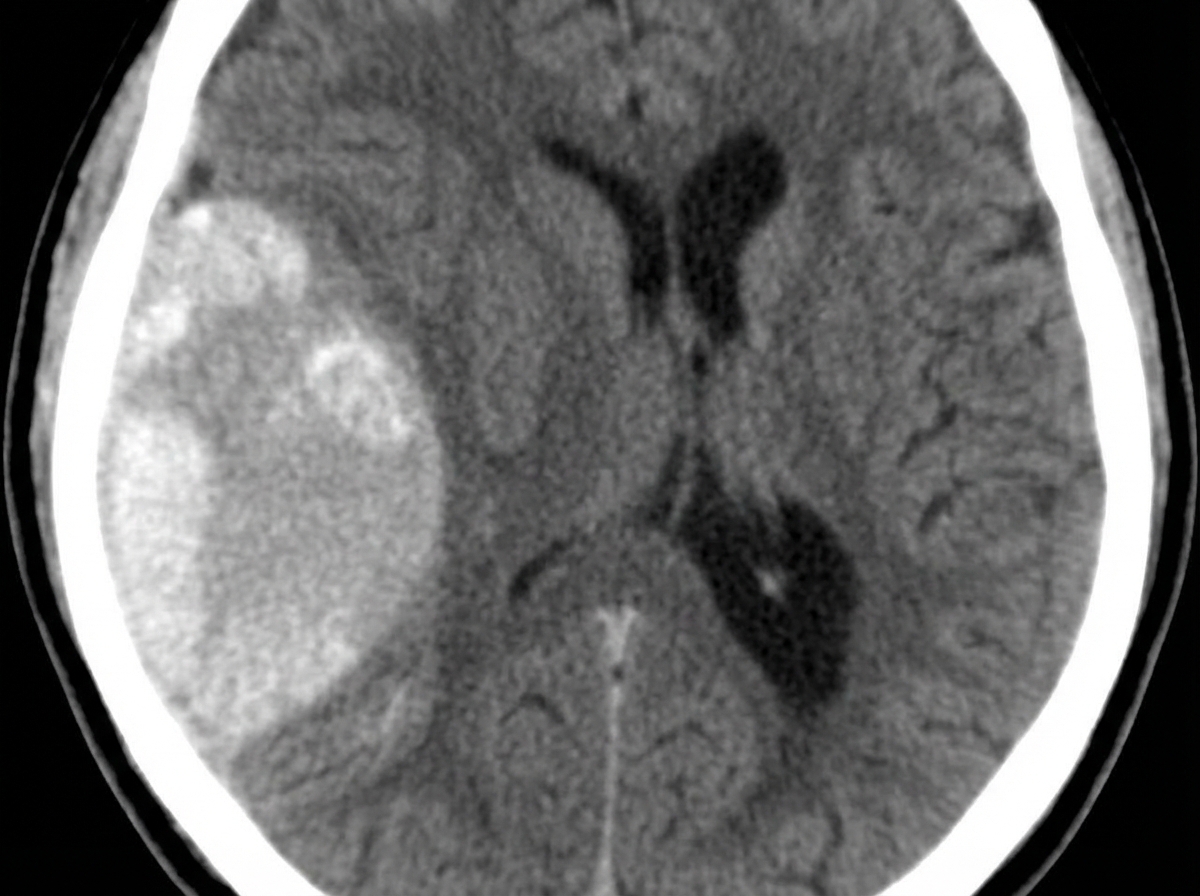
A 23-year-old man presents with a blunt force injury to the head from a baseball bat. He is currently unconscious, although his friends say he was awake and speaking with them en route to the hospital. He has no significant past medical history and takes no current medications. The vital signs include: temperature 37.0°C (98.6°F), blood pressure 165/85 mm Hg, pulse 50/min, and respiratory rate 19/min. On physical examination, there is a blunt force injury to the left temporoparietal region approximately 10.1–12.7 cm (4–5 in) in diameter. There is anisocoria of the left pupil, which is unresponsive to light. The patient is intubated and fluid resuscitation is initiated. A noncontrast computed tomography (CT) scan of the head is acquired and shown in the exhibit (see image). Which of the following is the most appropriate medical treatment for this patient?
A 26-year-old G1P0 woman at 32-weeks gestation presents for follow-up ultrasound. She was diagnosed with gestational diabetes during her second trimester, but admits to poor glucose control and non-adherence to insulin therapy. Fetal ultrasound reveals an asymmetric, enlarged interventricular septum, left ventricular outflow tract obstruction, and significantly reduced ejection fraction. Which of the following is the most appropriate step in management after delivery?
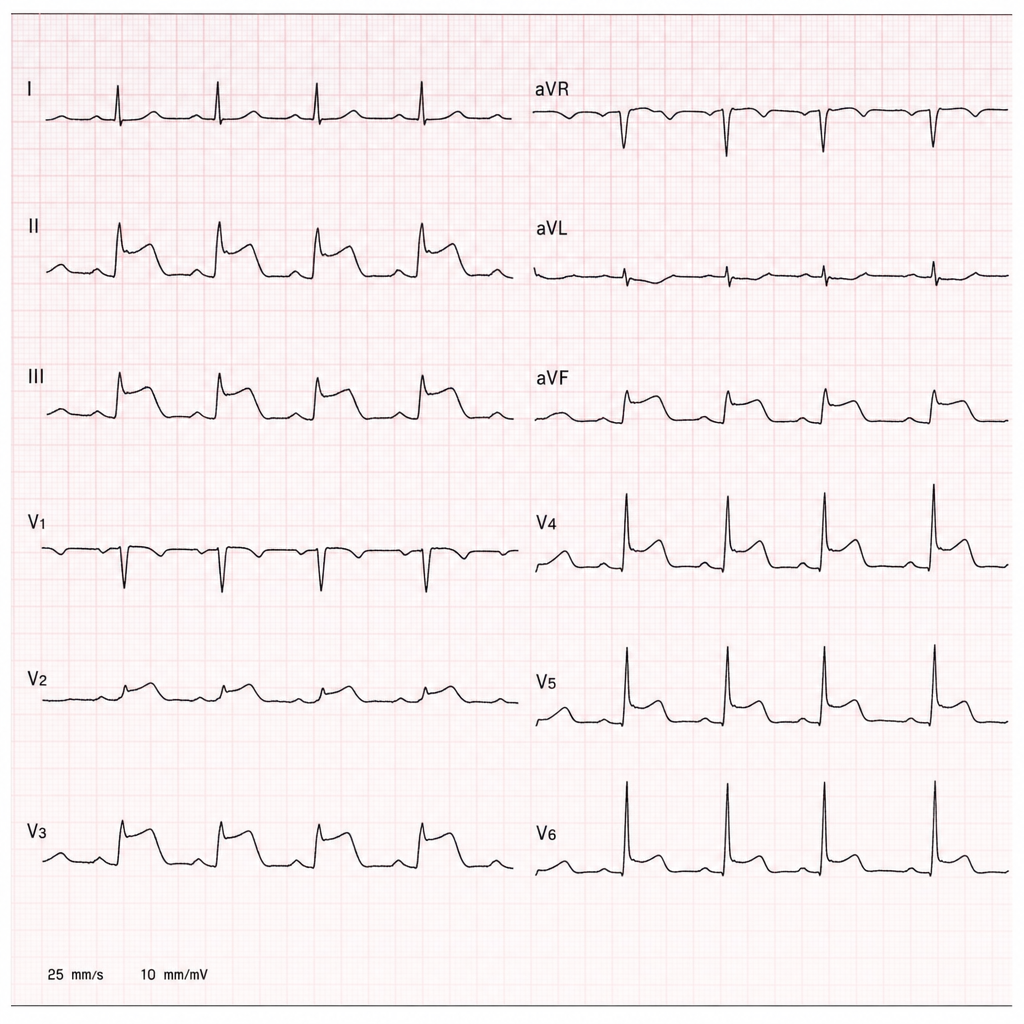
A 58-year-old man with hypertension and hyperlipidemia is brought to the emergency department by ambulance after collapsing at home. His wife states he complained of sudden severe chest pain radiating to the left arm 40 minutes ago, then became diaphoretic and lost consciousness briefly. On arrival, BP is 88/60 mmHg, HR 112 bpm, RR 22/min, SpO2 94% on room air. The ECG shown demonstrates 4 mm ST-segment elevation in leads II, III, and aVF with reciprocal changes in I and aVL. IV access is established, aspirin 325 mg has been given, and oxygen is being administered. The nearest percutaneous coronary intervention-capable facility is 25 minutes away. Which of the following is the most appropriate next step?
A 38-year-old previously healthy woman develops septic shock from necrotizing fasciitis of the lower extremity. Despite three debridements, broad-spectrum antibiotics (vancomycin, meropenem, clindamycin), IVIG, and aggressive critical care support, she develops refractory shock requiring norepinephrine 1.2 mcg/kg/min, vasopressin 0.04 units/min, and epinephrine 0.1 mcg/kg/min. Lactate is 15 mmol/L. Surgical team recommends hemipelvectomy as last option for source control. Family is devastated. ICU team notes SOFA score of 18. Synthesize an approach to management and decision-making.
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app