
Sepsis — MCQs

On this page
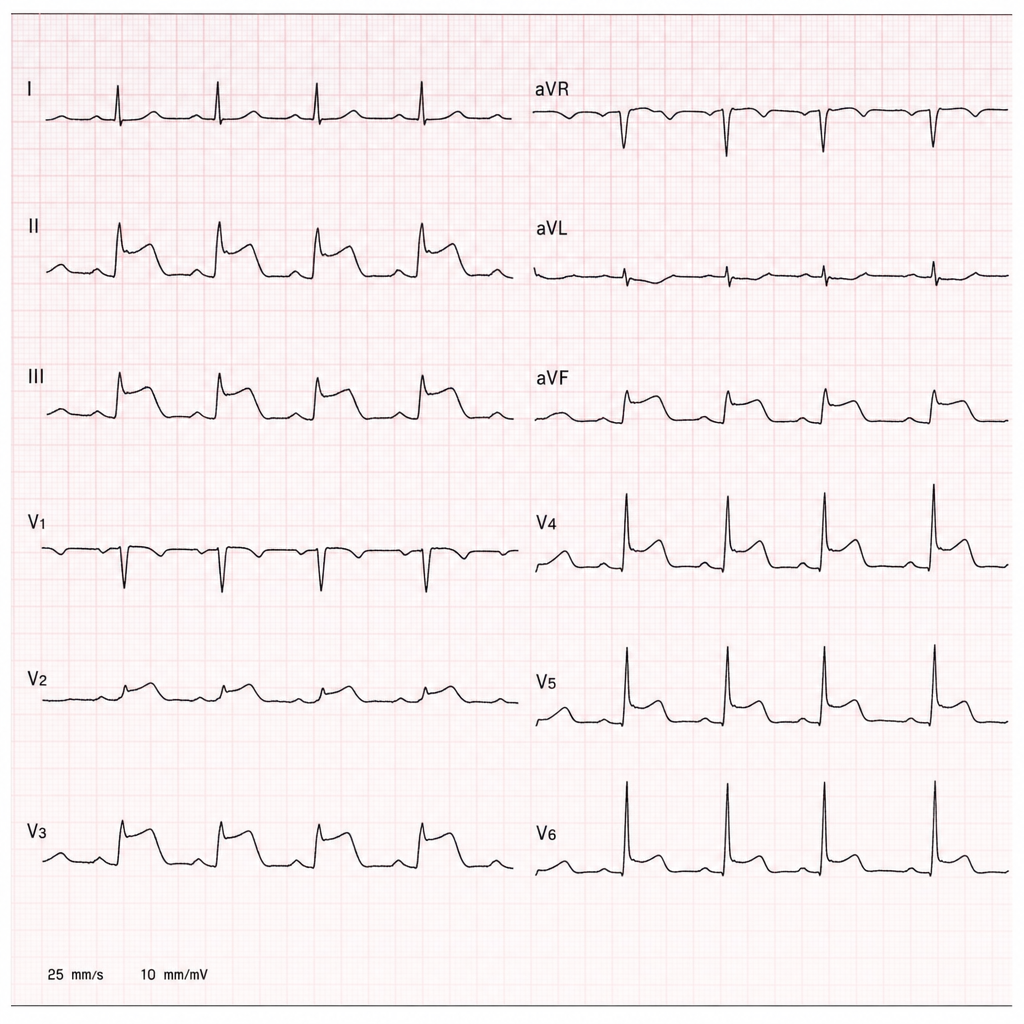
A 58-year-old man with hypertension and hyperlipidemia is brought to the emergency department by ambulance after collapsing at home. His wife states he complained of sudden severe chest pain radiating to the left arm 40 minutes ago, then became diaphoretic and lost consciousness briefly. On arrival, BP is 88/60 mmHg, HR 112 bpm, RR 22/min, SpO2 94% on room air. The ECG shown demonstrates 4 mm ST-segment elevation in leads II, III, and aVF with reciprocal changes in I and aVL. IV access is established, aspirin 325 mg has been given, and oxygen is being administered. The nearest percutaneous coronary intervention-capable facility is 25 minutes away. Which of the following is the most appropriate next step?
A 38-year-old previously healthy woman develops septic shock from necrotizing fasciitis of the lower extremity. Despite three debridements, broad-spectrum antibiotics (vancomycin, meropenem, clindamycin), IVIG, and aggressive critical care support, she develops refractory shock requiring norepinephrine 1.2 mcg/kg/min, vasopressin 0.04 units/min, and epinephrine 0.1 mcg/kg/min. Lactate is 15 mmol/L. Surgical team recommends hemipelvectomy as last option for source control. Family is devastated. ICU team notes SOFA score of 18. Synthesize an approach to management and decision-making.
A 52-year-old woman with septic shock from intra-abdominal infection undergoes emergency exploratory laparotomy for perforated diverticulitis with fecal peritonitis. Surgery reveals extensive contamination requiring damage control approach. Postoperatively, she requires norepinephrine 0.8 mcg/kg/min plus vasopressin 0.04 units/min, has lactate of 8.5 mmol/L, temperature 35.2°C, INR 2.8, pH 7.18, and base deficit -12. Planned return to OR is in 48 hours. Evaluate the priority interventions to optimize outcome.
A 70-year-old man with recently diagnosed small cell lung cancer presents with septic shock from pneumonia. After initial resuscitation, he requires norepinephrine 0.6 mcg/kg/min and has a lactate of 7.8 mmol/L. His SOFA score is 14. The family requests 'everything be done,' but the patient had previously told his oncologist he would not want prolonged intensive care if his cancer prognosis was poor. Staging shows extensive-stage disease. The ICU team debates goals of care. What represents the most ethically appropriate approach to decision-making?
A 63-year-old man with septic shock from pneumonia has been on mechanical ventilation for 48 hours. He received 6 liters of crystalloid in the first 24 hours and requires norepinephrine 0.25 mcg/kg/min to maintain MAP of 68 mmHg. Physical examination shows bilateral crackles, jugular venous distension, and 2+ pitting edema. Chest X-ray shows bilateral infiltrates and pulmonary edema. PaO2/FiO2 ratio is 180. CVP is 16 mmHg. What is the most appropriate fluid management strategy at this point?
Practice by Chapter
SIRS and sepsis definitions
Practice Questions
Early recognition of sepsis
Practice Questions
Initial resuscitation in sepsis
Practice Questions
Source identification and control
Practice Questions
Empiric antimicrobial therapy
Practice Questions
Fluid resuscitation strategies
Practice Questions
Vasopressors and inotropic support
Practice Questions
Blood culture technique and interpretation
Practice Questions
Sepsis-induced organ dysfunction management
Practice Questions
Septic shock management
Practice Questions
De-escalation strategies
Practice Questions
Biomarkers in sepsis management
Practice Questions
Sepsis bundles and quality metrics
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app