
Reperfusion strategies (fibrinolysis vs PCI) — MCQs

A 56-year-old man comes to the emergency department complaining of substernal chest pain that radiates to the left shoulder. Electrocardiogram (EKG) demonstrates ST-elevations in leads II, III, and aVF. The patient subsequently underwent catheterization with drug-eluting stent placement with stabilization of his condition. On post-operative day 3, the patient experiences stabbing chest pain that is worse with inspiration, diaphoresis, and general distress. His temperature is 98.7°F (37.1°C), blood pressure is 145/97mmHg, pulse is 110/min, and respirations are 23/min. EKG demonstrates diffuse ST-elevations. What is the best treatment for this patient?
A 53-year-old man with a past medical history significant for hyperlipidemia, hypertension, and hyperhomocysteinemia presents to the emergency department complaining of 10/10 crushing, left-sided chest pain radiating down his left arm and up his neck into the left side of his jaw. His ECG shows ST-segment elevation in leads V2-V4. He is taken to the cardiac catheterization laboratory for successful balloon angioplasty and stenting of a complete blockage in his left anterior descending coronary artery. Echocardiogram the following day shows decreased left ventricular function and regional wall motion abnormalities. A follow-up echocardiogram 14 days later shows a normal ejection fraction and no regional wall motion abnormalities. This post-infarct course illustrates which of the following concepts?
A 79-year-old man is brought to the emergency department after he noted the abrupt onset of weakness accompanied by decreased sensation on his left side. His symptoms developed rapidly, peaked within 1 minute, and began to spontaneously resolve 10 minutes later. Upon arrival in the emergency room 40 minutes after the initial onset of symptoms, they had largely resolved. The patient has essential hypertension, type 2 diabetes mellitus, chronic obstructive pulmonary disease, and a 50 pack-year smoking history. He also had an ST-elevation myocardial infarction 3 years ago. His brain CT scan without contrast is reported as normal. Carotid duplex ultrasonography reveals 90% stenosis of the right internal carotid. His transthoracic echocardiogram does not reveal any intracardiac abnormalities. Which of the following interventions is most appropriate for this patient's condition?
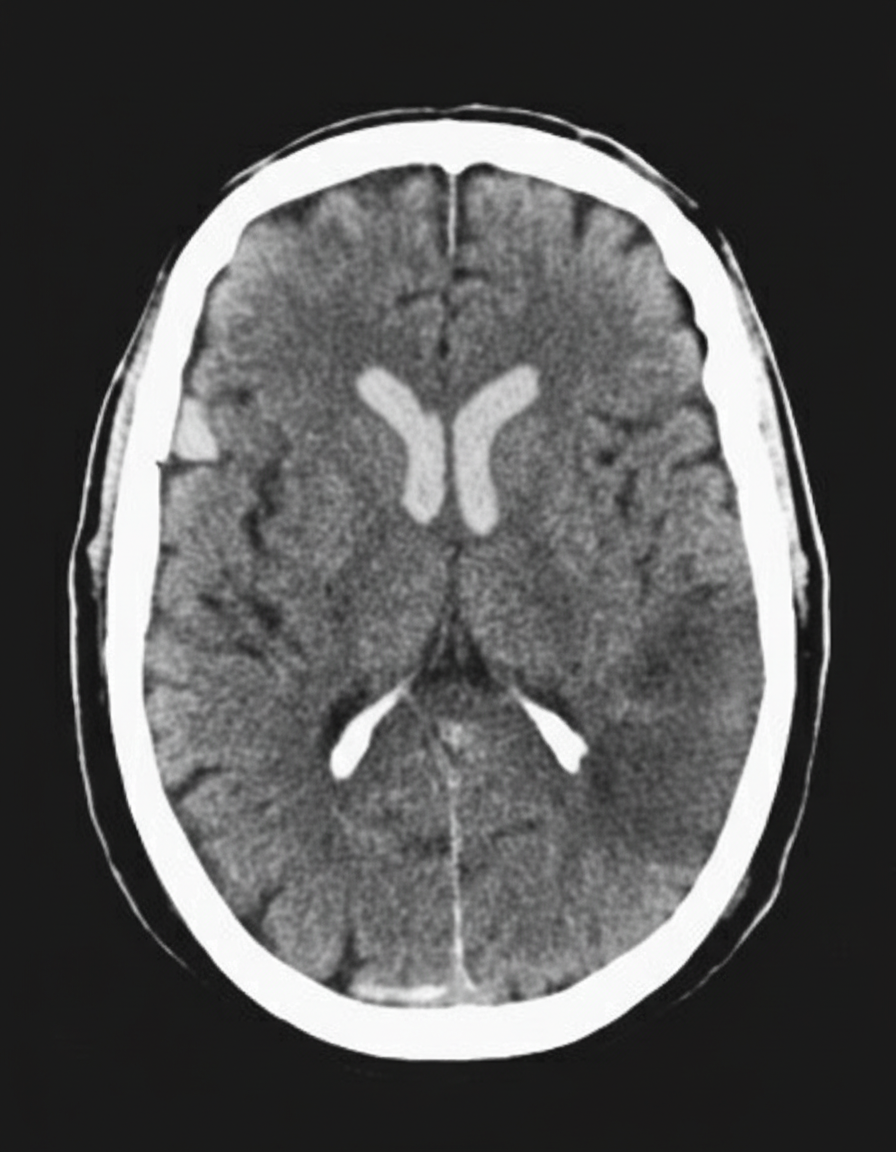
A 45-year-old man presents to the emergency department with complaints of right-sided weakness and slurring of speech for 1 hour. There is no history of head trauma, myocardial infarction, recent surgery, gastrointestinal or urinary bleeding. He has hypertension, chronic atrial fibrillation, and a 20 pack-year cigarette smoking history. The medication list includes valsartan and rivaroxaban. The vital signs include: blood pressure 180/92 mm Hg, pulse 144/min and irregular, and temperature 37.2°C (99.0°F). On physical examination, there is a facial asymmetry with a deviation of angle of mouth to the left side on smiling. Muscle strength is reduced in both upper and lower limbs on the right side while on the left side it’s normal. Random blood glucose is 104 mg/dL. A complete blood count is normal. A CT scan of the head is shown in the image. What is the most appropriate next step in the management of this patient?
A 54-year-old woman comes to the emergency department because of two episodes of bright red blood per rectum within the past day. She has a history of migraine, which is treated prophylactically with verapamil. She appears well and is hemodynamically stable. Cardiac exam reveals a regular heart rate without any murmurs or gallops. Lungs are clear to auscultation. Her abdomen is mildly tender without rebound or guarding. Digital rectal examination shows fresh blood on the glove. Laboratory studies show: Hemoglobin 10.4 g/dL Leukocyte count 5,000/mm3 Platelet count 175,000/mm3 Partial thromboplastin time 35 seconds Serum Na+ 140 mEq/L K+ 3.7 mEq/L Cl- 101 mEq/L HCO3- 25 mEq/L Mg2+ 1.8 mEq/L A routine ECG shows a heart rate of 75/min, a normal axis, PR interval of 280 ms, QRS interval of 80 ms with a QRS complex following each p wave, and no evidence of ischemic changes. Which of the following is the most appropriate next step in management with respect to this patient's cardiovascular workup?
A 69-year-old man is scheduled to undergo radical retropubic prostatectomy for prostate cancer in 2 weeks. He had a myocardial infarction at the age of 54 years. He has a history of GERD, unstable angina, hyperlipidemia, and severe osteoarthritis in the left hip. He is unable to climb up stairs or walk fast because of pain in his left hip. He had smoked one pack of cigarettes daily for 30 years but quit 25 years ago. He drinks one glass of wine daily. Current medications include aspirin, metoprolol, lisinopril, rosuvastatin, omeprazole, and ibuprofen as needed. His temperature is 36.4°C (97.5°F), pulse is 90/min, and blood pressure is 136/88 mm Hg. Physical examination shows no abnormalities. A 12-lead ECG shows Q waves and inverted T waves in leads II, III, and aVF. His B-type natriuretic protein is 84 pg/mL (N < 125). Which of the following is the most appropriate next step in management to assess this patient's perioperative cardiac risk?
A 70-year-old man is brought to the emergency room with complaints of severe substernal chest pain for the last hour. The pain started suddenly, and the patient describes the pain as “going into the shoulder”. The patient took aspirin at home and has been given multiple doses of sublingual nitroglycerin, but the pain has not subsided. He has a blood pressure of 112/84 mm Hg, the pulse is 63/min, the respiratory rate is 18/min, and the temperature is 36.9°C (98.0°F). Cardiac auscultation reveals normal S1 and S2 sounds, however, an additional S4 sound is heard. The patient is sweating profusely, and the lungs are clear to auscultation. No jugular venous distension or pedal edema is observed. His initial ECG shows ST elevation in leads II, III, and aVF. Which of the following will likely have the most benefit in this patient?
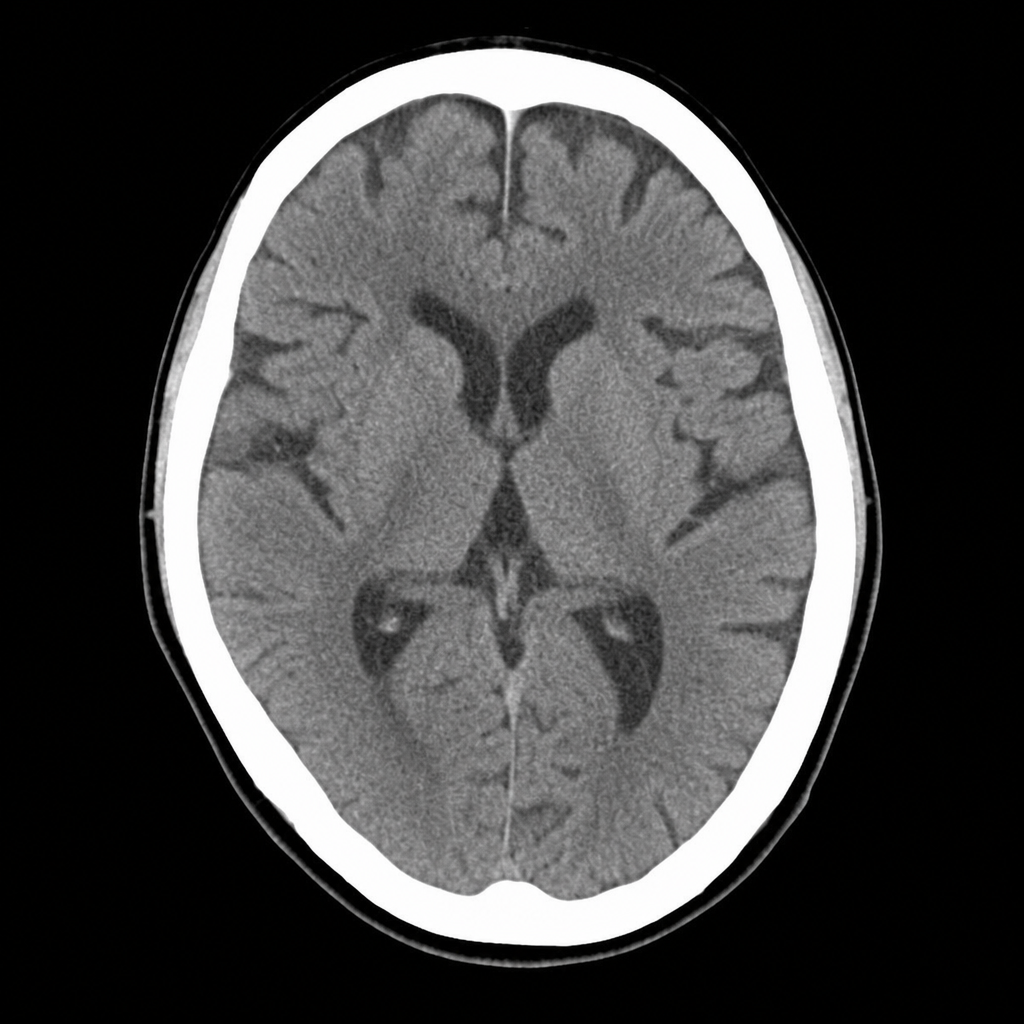
A 67-year-old man with hypertension and type 2 diabetes is brought to the ED by his wife, who noticed he developed sudden right-sided facial droop and slurred speech approximately 2 hours ago. On arrival, blood pressure is 188/104 mmHg, heart rate 82 bpm, oxygen saturation 97% on room air. Neurological examination reveals right facial weakness, dysarthria, and mild right arm drift. NIHSS score is 7. A non-contrast CT head is performed and shown above. No hemorrhage, early infarct signs, or mass lesion is identified. The patient takes metformin and lisinopril; no anticoagulants. Which of the following is the most appropriate immediate next step?
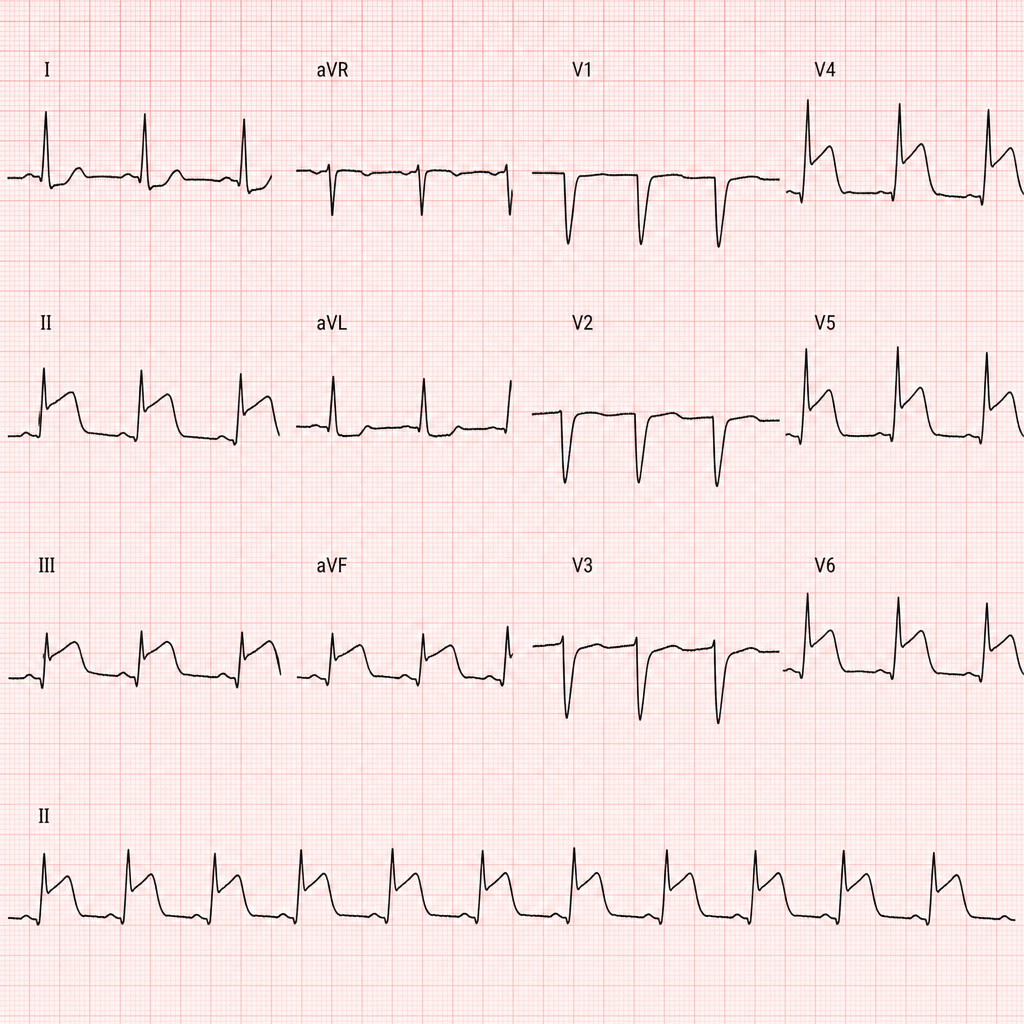
A 67-year-old man with hypertension and hyperlipidemia presents to the emergency department with 45 minutes of crushing substernal chest pain radiating to his left arm. He is diaphoretic and pale. Vital signs: BP 88/60 mmHg, HR 112 bpm, RR 20/min, SpO2 94% on room air. PCI is immediately available. An ECG is obtained and shown above. Two large-bore IVs are placed. Which of the following is the most appropriate immediate next step?
A 70-year-old man with diabetes, hypertension, and chronic kidney disease (eGFR 35 mL/min/1.73m²) presents with NSTEMI. Troponin is elevated at 8.5 ng/mL. ECG shows 2mm ST depression in V2-V5. GRACE score is 165 (high risk). He is hemodynamically stable. Cardiologist recommends early invasive strategy within 24 hours. Nephrologist is concerned about contrast-induced nephropathy potentially requiring dialysis. Patient is on metformin. Evaluate the management strategy integrating multiple specialist perspectives and evidence.
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app