
Post-MI secondary prevention — MCQs

A 69-year-old man presents for a general follow up appointment. He states that he is doing well and wants to be sure he is healthy. The patient’s past medical history is significant for type II diabetes mellitus, peripheral vascular disease, and hypertension. His current medications include metformin, glyburide, lisinopril, metoprolol and hydrochlorothiazide. His blood pressure is 130/90 mmHg and pulse is 80/min. A fasting lipid panel was performed last week demonstrating an LDL of 85 mg/dL and triglycerides of 160 mg/dL. The patient states that he has not experienced any symptoms since his last visit. The patient’s blood glucose at this visit is 100 mg/dL. Which of the following is recommended in this patient?
A 55-year-old man comes to the physician because of a 4-month history of episodic, pressure-like chest pain. The chest pain occurs when he is walking up stairs and improves with rest. He has hypertension and type 2 diabetes mellitus. His father died from a myocardial infarction at the age of 50 years. Current medications include hydrochlorothiazide and metformin. His pulse is 85/min, respirations are 12/min, and blood pressure is 140/90 mm Hg. Cardiac examination shows normal heart sounds without any murmurs, rubs, or gallops. An ECG shows high amplitude of the S wave in lead V3. An exercise stress test is performed but stopped after 4 minutes because the patient experiences chest pain. An ECG obtained during the stress test shows sinus tachycardia and ST-segment depressions in leads V1–V4. Which of the following is the most appropriate long-term pharmacotherapy to reduce the frequency of symptoms in this patient?
A 64-year-old man presents to his physician for a scheduled follow-up visit. He has chronic left-sided heart failure with systolic dysfunction. His current regular medications include captopril and digoxin, which were started after his last episode of symptomatic heart failure approximately 3 months ago. His last episode of heart failure was accompanied by atrial fibrillation, which followed an alcohol binge over a weekend. Since then he stopped drinking. He reports that he has no current symptoms at rest and is able to perform regular physical exercise without limitation. On physical examination, mild bipedal edema is noted. The physician suggested to him that he should discontinue digoxin and continue captopril and scheduled him for the next follow-up visit. Which of the following statements best justifies the suggestion made by the physician?
A 72-year-old man presents to the outpatient clinic today. He has New York Heart Association class III heart failure. His current medications include captopril 20 mg, furosemide 40 mg, potassium chloride 10 mg twice daily, rosuvastatin 20 mg, and aspirin 81 mg. He reports that he generally feels well and has not had any recent worsening of his symptoms. His blood pressure is 132/85 mm Hg and heart rate is 84/min. Physical examination is unremarkable except for trace pitting edema of the bilateral lower extremities. What other medication should be added to his heart failure regimen?
A 49-year-old man with a past medical history of hypertension on amlodipine presents to your office to discuss ways to lessen his risk of complications from heart disease. After a long discussion, he decides to significantly decrease his intake of trans fats in an attempt to lower his risk of coronary artery disease. Which type of prevention is this patient initiating?
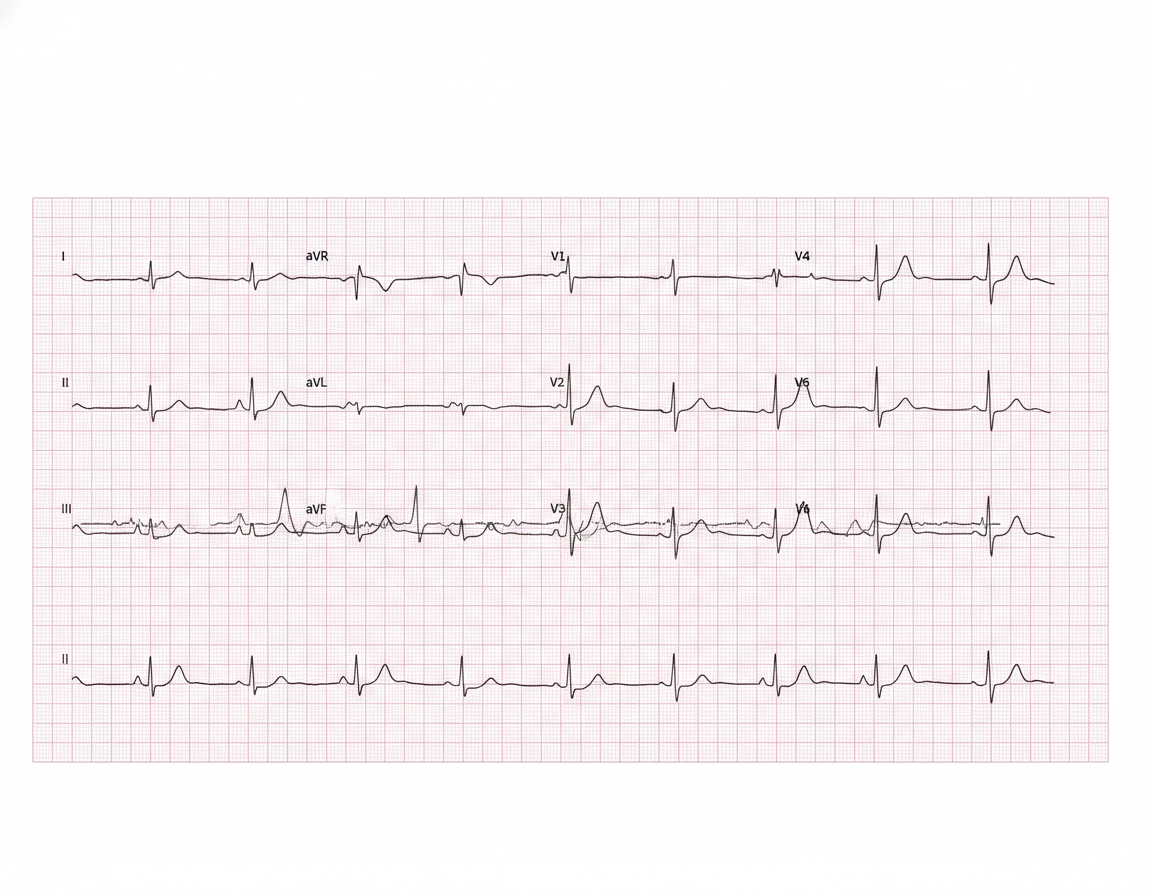
A 57-year-old man presents to the emergency department for evaluation of slurred speech and left arm and leg weakness over the last 3 hours. History reveals hypertension that is being treated with hydrochlorothiazide. Vital signs include: blood pressure of 110/70 mm Hg, heart rate 104/min, respiratory rate 18/min, and temperature 36.6°C (98.0°F). Physical examination reveals 2/5 strength in both left upper and lower extremities. After 2 hours, the patient’s symptoms suddenly disappear. An electrocardiogram (ECG) is obtained (see image). Which of the following medications could prevent ischemic attacks in this patient in the future?
A 56-year-old woman comes to the physician for follow-up after a measurement of elevated blood pressure at her last visit three months ago. She works as a high school teacher at a local school. She says that she mostly eats cafeteria food and take-out. She denies any regular physical activity. She does not smoke or use any recreational drugs. She drinks 2 to 3 glasses of wine per day. She has hypercholesterolemia for which she takes atorvastatin. Her height is 165 cm (5 ft 5 in), weight is 82 kg (181 lb), and BMI is 30.1 kg/m2. Her pulse is 67/min, respirations are 18/min, and blood pressure is 152/87 mm Hg on the right arm and 155/92 mm Hg on the left arm. She would like to try lifestyle modifications to improve her blood pressure before considering pharmacologic therapy. Which of the following lifestyle modifications is most likely to result in the greatest reduction of this patient's systolic blood pressure?
A 73-year-old man presents to the outpatient clinic complaining of chest pain with exertion. He states that resting for a few minutes usually resolves the chest pain. Currently, he takes 81 mg of aspirin daily. He has a blood pressure of 127/85 mm Hg and heart rate of 75/min. Physical examination reveals regular heart sounds and clear lung sounds bilateral. Which medication regimen below should be added?
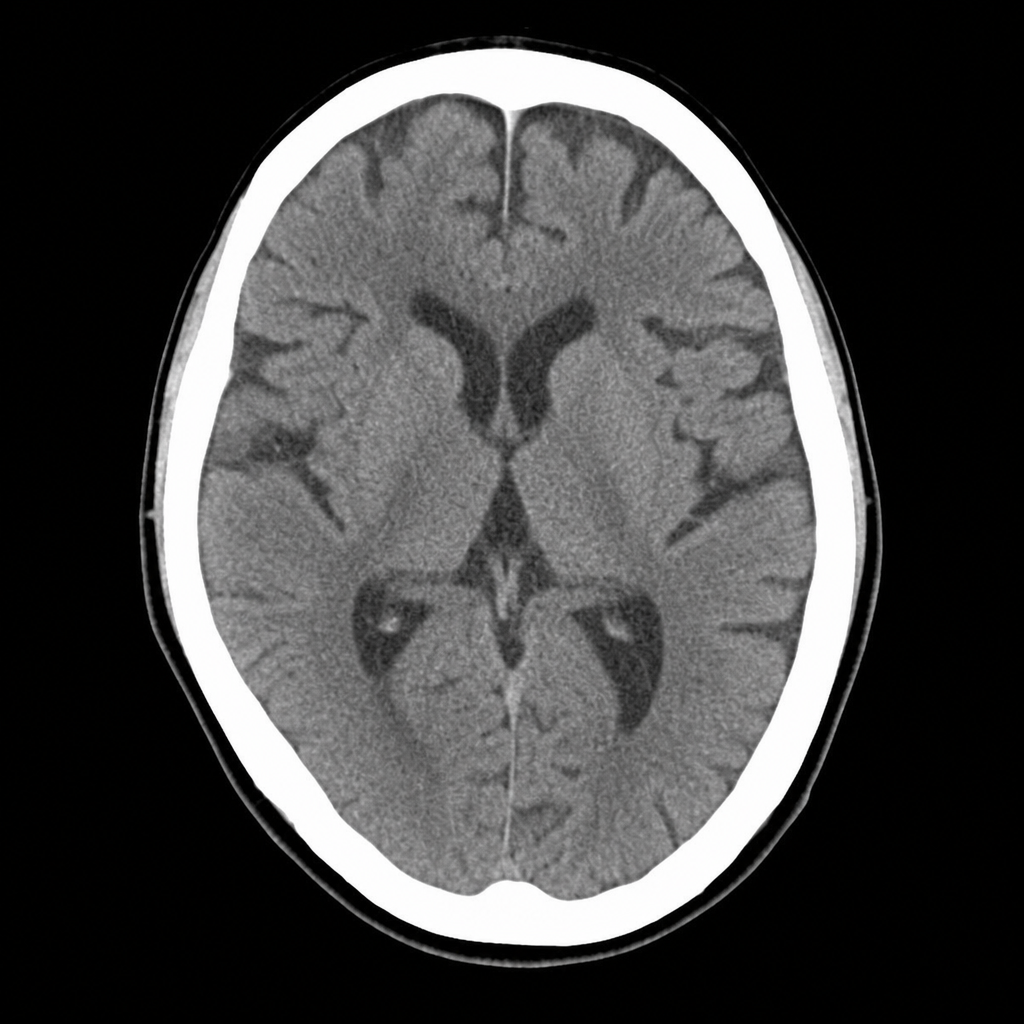
A 67-year-old man with hypertension and type 2 diabetes is brought to the ED by his wife, who noticed he developed sudden right-sided facial droop and slurred speech approximately 2 hours ago. On arrival, blood pressure is 188/104 mmHg, heart rate 82 bpm, oxygen saturation 97% on room air. Neurological examination reveals right facial weakness, dysarthria, and mild right arm drift. NIHSS score is 7. A non-contrast CT head is performed and shown above. No hemorrhage, early infarct signs, or mass lesion is identified. The patient takes metformin and lisinopril; no anticoagulants. Which of the following is the most appropriate immediate next step?
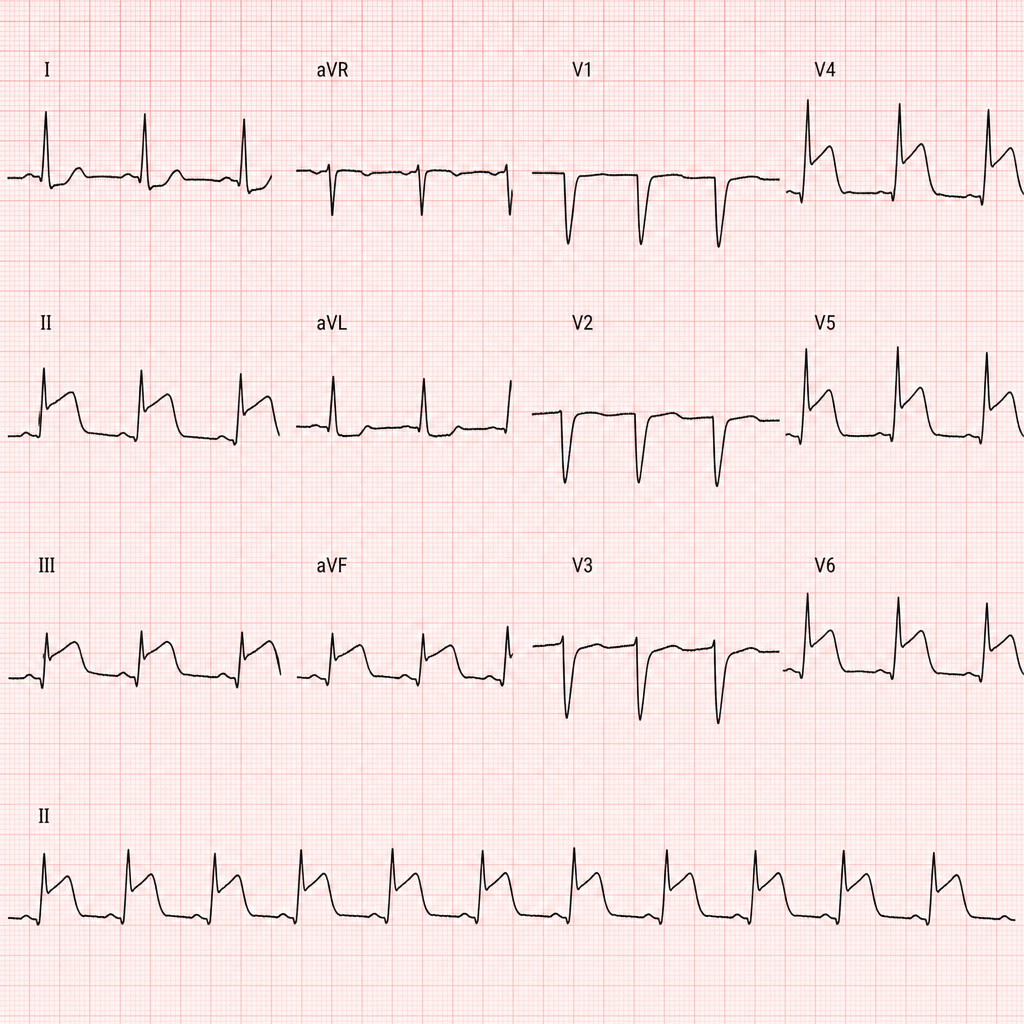
A 67-year-old man with hypertension and hyperlipidemia presents to the emergency department with 45 minutes of crushing substernal chest pain radiating to his left arm. He is diaphoretic and pale. Vital signs: BP 88/60 mmHg, HR 112 bpm, RR 20/min, SpO2 94% on room air. PCI is immediately available. An ECG is obtained and shown above. Two large-bore IVs are placed. Which of the following is the most appropriate immediate next step?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app