
Initial assessment and triage — MCQs

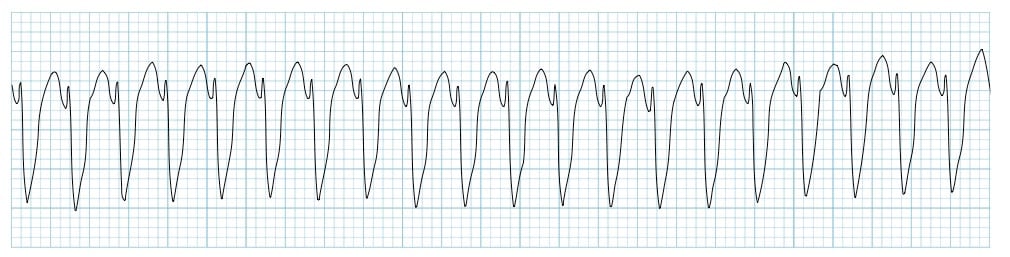
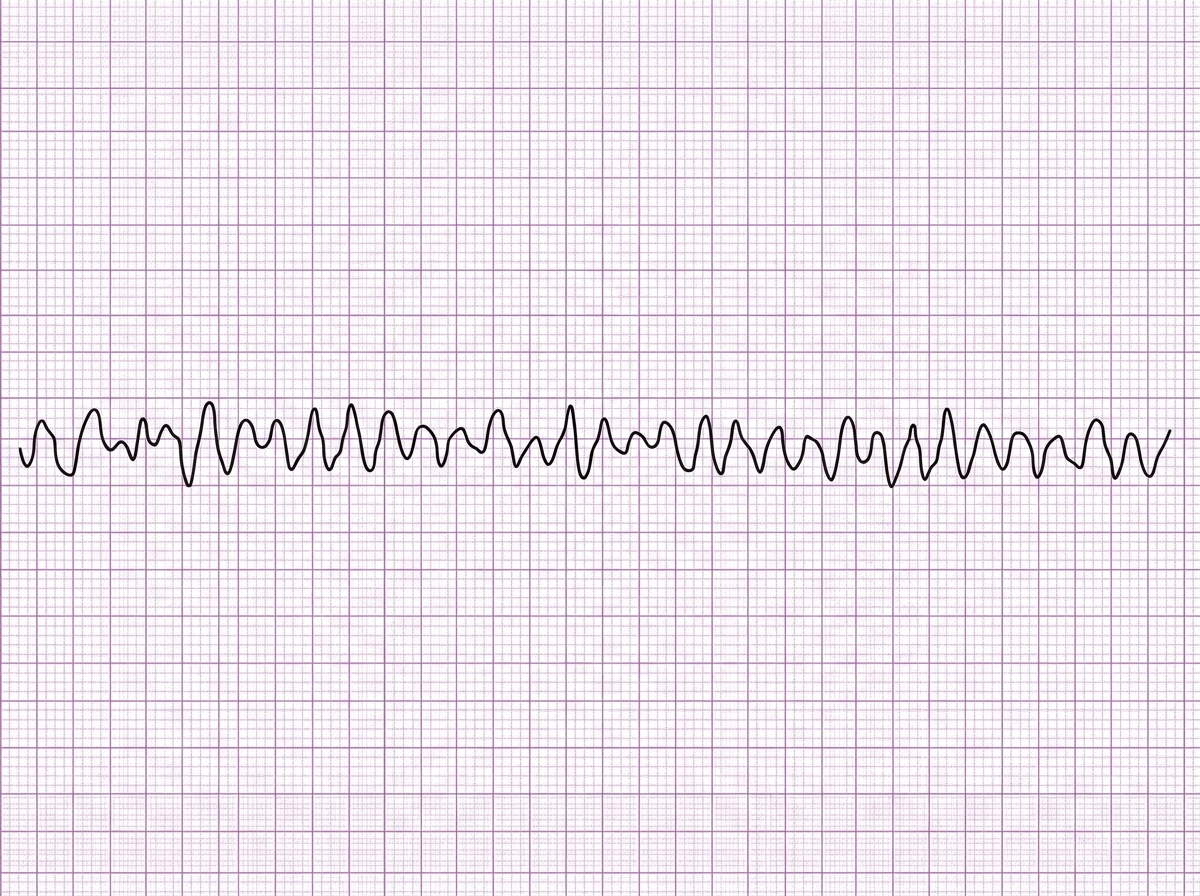
Two days after admission for myocardial infarction and subsequent coronary angioplasty, a 65-year-old man becomes distressed and diaphoretic in the cardiac intensive care unit. Suddenly he is no longer responsive. Pulse oximetry does not show a tracing. He has a history of hypertension and depression. Prior to his admission, his medication included ramipril and aripiprazole. Examination shows no carotid pulse. An ECG is shown. After beginning chest compressions, which of the following is the most appropriate step in management of the patient?
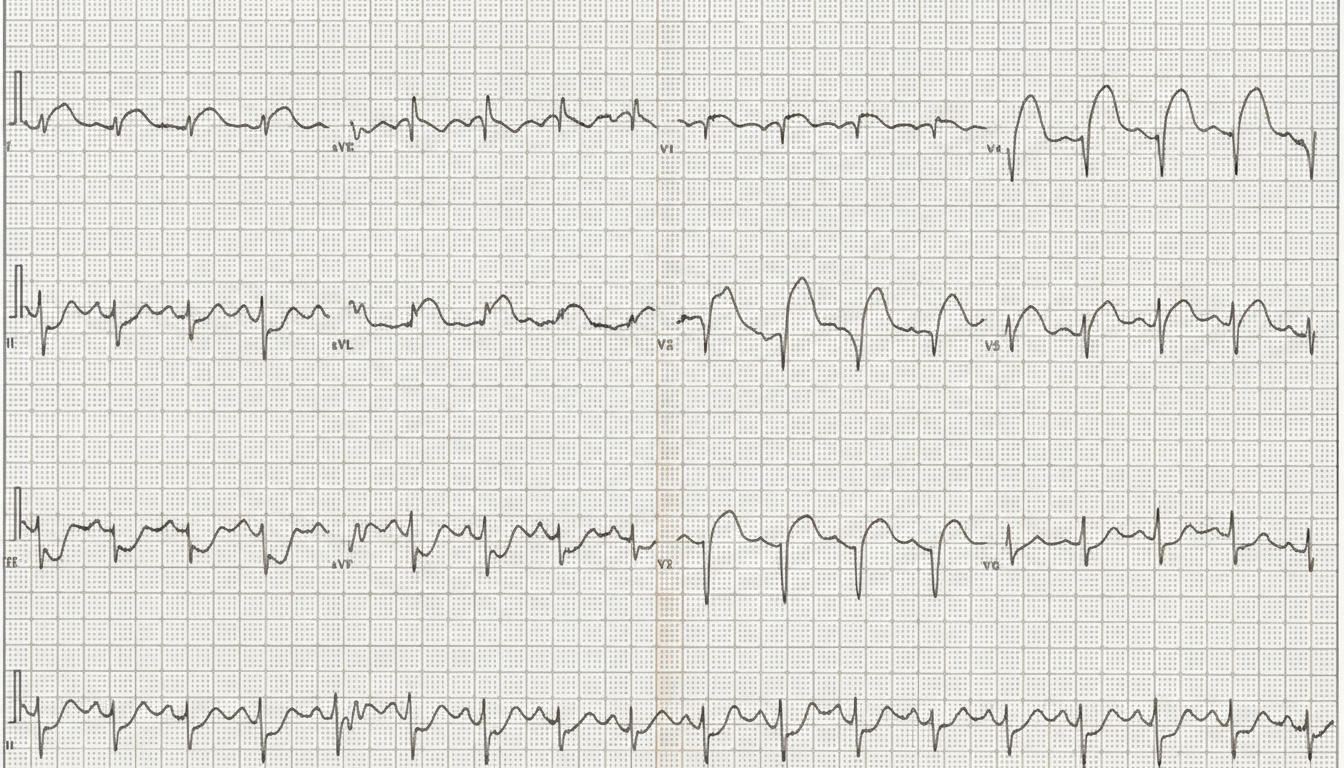
A 57-year-old man with a known angina pectoris starts to experience a severe burning retrosternal pain that radiates to his left hand. After 2 consecutive doses of sublingual nitroglycerin taken 5 minutes apart, there is no improvement in his symptoms, and the patient calls an ambulance. Emergency medical service arrives within 10 minutes and begins evaluation and prehospital management. The vital signs include: blood pressure 85/50 mm Hg, heart rate 96/min, respiratory rate 19/min, temperature 37.1℃ (98.9℉), and SpO2 89% on ambient air. Oxygen supply and intravenous access are established. An ECG shows the findings in the given image. Which of the following is a part of a proper further prehospital management strategy for this patient?
A 66-year-old man comes to the emergency department because of a 1-day history of chest pain, palpitations, and dyspnea on exertion. He had a similar episode 3 days ago and was diagnosed with an inferior wall myocardial infarction. He was admitted and a percutaneous transluminal coronary angioplasty was successfully done that day. A fractional flow reserve test during the procedure showed complete resolution of the stenosis. Laboratory tests including serum glucose, lipids, and blood count were within normal limits. He was discharged the day after the procedure on a drug regimen of aspirin, simvastatin, and isosorbide dinitrate. At the time of discharge, he had no chest pain or dyspnea. Presently, his vitals are normal and ECG at rest shows new T-wave inversion. Which of the following is the most reliable test for rapidly establishing the diagnosis in this patient?
A 66-year-old man presents to the emergency department with a 3-hour history of crushing chest pain radiating to the left shoulder and neck. Patient states that the pain began suddenly when he was taking a walk around the block and has not improved with rest. He also mentions difficulty breathing and prefers to sit leaning forward. He denies ever having similar symptoms before. Past medical history is significant for hypertension, diagnosed 10 years ago, and hyperlipidemia diagnosed 8 years ago. Current medications are atorvastatin. Patient is also prescribed hydrochlorothiazide as an antihypertensive but is not compliant because he says it makes him urinate too often. Vitals show a blood pressure of 152/90 mm Hg, pulse of 106/min, respirations of 22/min and oxygen saturation of 97% on room air. On physical exam, patient is profusely diaphoretic and hunched over in distress. Cardiac exam is unremarkable and lungs are clear to auscultation. During your examination, the patient suddenly becomes unresponsive and a pulse cannot be palpated. A stat ECG shows the following (see image). Which of the following is the next best step in management?
A cardiologist is studying how a new virus that infects the heart affects the electrical conduction system of the cardiac myocytes. He decides to obtain electrocardiograms on patients with this disease in order to see how the wave patterns and durations change over time. While studying these records, he asks a medical student who is working with him to interpret the traces. Specifically, he asks her to identify the part that represents initial ventricular depolarization. Which of the following characteristics is most consistent with this feature of the electrocardiogram?
A 67-year-old man presents to the emergency department for squeezing and substernal chest pain. He states that he was at home eating dinner when his symptoms began. The patient has a past medical history of diabetes, hypertension, and dyslipidemia. He is currently taking atorvastatin, lisinopril, insulin, metformin, metoprolol, and aspirin. Six days ago he underwent percutaneous coronary intervention. His temperature is 99.5°F (37.5°C), blood pressure is 197/118 mmHg, pulse is 120/min, respirations are 17/min, and oxygen saturation is 98% on room air. Physical exam reveals an uncomfortable elderly man who is sweating. An ECG is ordered. Which of the following is the best next step in management for this patient?
Serum studies show a troponin T concentration of 6.73 ng/mL (N < 0.01), and fingerstick blood glucose concentration of 145 mg/dL. The cardiac catheterization team is activated. Treatment with unfractionated heparin, aspirin, ticagrelor, and sublingual nitroglycerin is begun, and the patient's pain subsides. His temperature is 37.3°C (99.1°F), pulse is 65/min, respirations are 23/min, and blood pressure is 91/60 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 96%. Which of the following is the most appropriate additional pharmacotherapy?
A 60-year-old man presents to the emergency department with progressive dyspnea for the last 3 weeks. He complains of shortness of breath while lying flat and reports nighttime awakenings due to shortness of breath for the same duration. The patient has been a smoker for the last 30 years. Past medical history is significant for myocardial infarction 7 months ago. Current medications include metoprolol, aspirin, and rosuvastatin, but the patient is noncompliant with his medications. His temperature is 37.2°C (98.9°F), the blood pressure is 150/115 mm Hg, the pulse is 110/min, and the respiratory rate is 24/min. Oxygen saturation on room air is 88%. Chest auscultation reveals bilateral crackles and an S3 gallop. On physical examination, the cardiac apex is palpated in left 6th intercostal space. Bilateral pitting edema is present, and the patient is in moderate distress. Which of the following is the best next step in the management of the patient?
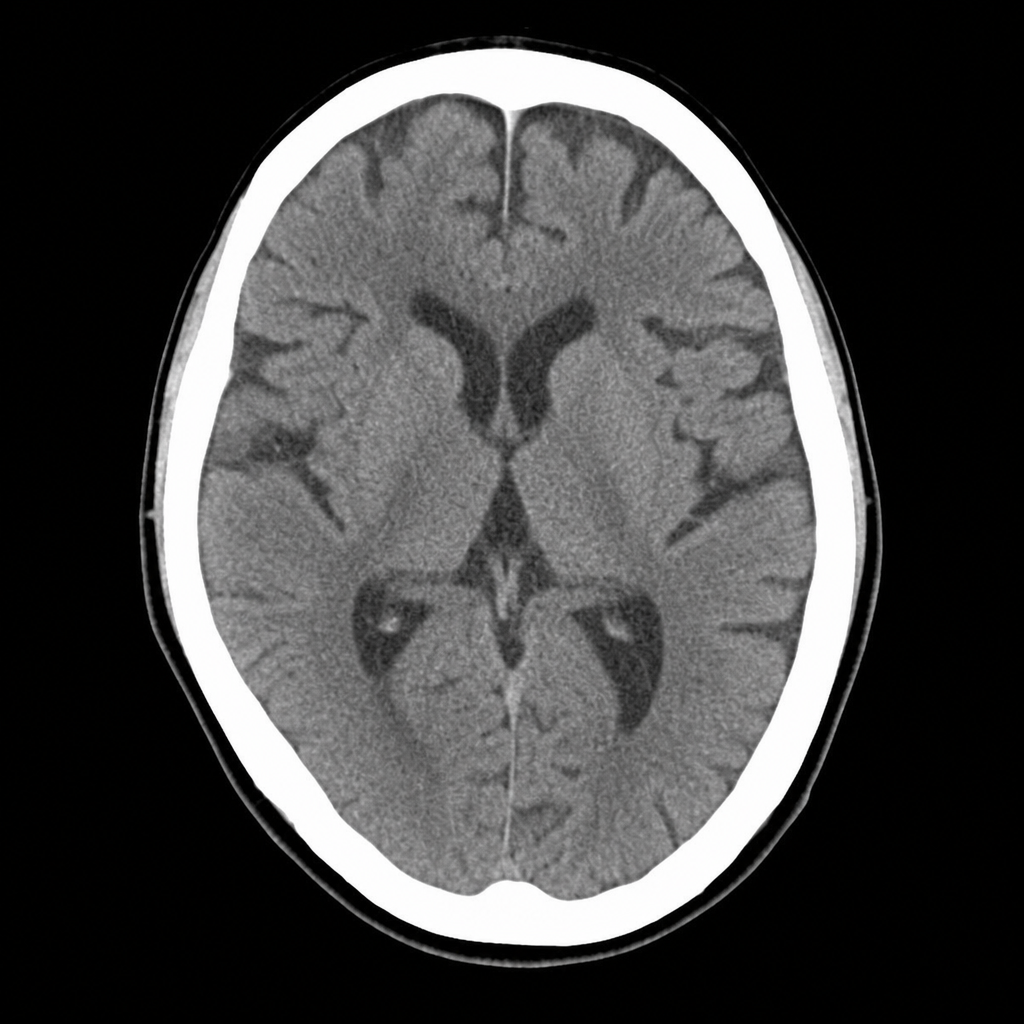
A 67-year-old man with hypertension and type 2 diabetes is brought to the ED by his wife, who noticed he developed sudden right-sided facial droop and slurred speech approximately 2 hours ago. On arrival, blood pressure is 188/104 mmHg, heart rate 82 bpm, oxygen saturation 97% on room air. Neurological examination reveals right facial weakness, dysarthria, and mild right arm drift. NIHSS score is 7. A non-contrast CT head is performed and shown above. No hemorrhage, early infarct signs, or mass lesion is identified. The patient takes metformin and lisinopril; no anticoagulants. Which of the following is the most appropriate immediate next step?
A 67-year-old man with hypertension and hyperlipidemia presents to the emergency department with 45 minutes of crushing substernal chest pain radiating to his left arm. He is diaphoretic and pale. Vital signs: BP 88/60 mmHg, HR 112 bpm, RR 20/min, SpO2 94% on room air. PCI is immediately available. An ECG is obtained and shown above. Two large-bore IVs are placed. Which of the following is the most appropriate immediate next step?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app