
ECG interpretation in MI — MCQs

A 53-year-old man with a past medical history significant for hyperlipidemia, hypertension, and hyperhomocysteinemia presents to the emergency department complaining of 10/10 crushing, left-sided chest pain radiating down his left arm and up his neck into the left side of his jaw. His ECG shows ST-segment elevation in leads V2-V4. He is taken to the cardiac catheterization laboratory for successful balloon angioplasty and stenting of a complete blockage in his left anterior descending coronary artery. Echocardiogram the following day shows decreased left ventricular function and regional wall motion abnormalities. A follow-up echocardiogram 14 days later shows a normal ejection fraction and no regional wall motion abnormalities. This post-infarct course illustrates which of the following concepts?
A 43-year-old woman presents to a physician with weakness and fatigue for a week. She mentions that she has been taking oral fluconazole for the last 4 weeks for the treatment of tinea capitis. She also says that she loves coffee and usually consumes 4–6 cups of coffee every day. On physical examination, her vital signs are stable and examination of all systems, including nervous system, is normal. Her laboratory evaluation reveals that her serum potassium level is 3.1 mmol/L (3.1 mEq/L). The physician orders an ECG. Which of the following findings is most likely to be present?
A 41-year-old woman presents to the emergency room with chest pain. She has had progressive substernal chest pain accompanied by weakness and mild shortness of breath for the past 2 hours. Her past medical history is notable for poorly controlled systemic lupus erythematosus (SLE), Sjogren syndrome, and interstitial lung disease. She was hospitalized last year with pericarditis presumed to be from SLE. Her temperature is 98.6°F (37°C), blood pressure is 106/56 mmHg, pulse is 132/min, and respirations are 26/min. On exam, the skin overlying the internal jugular vein fills at 9 cm above the sternal angle and distant heart sounds are appreciated. There is no friction rub. She is given 1000cc of intravenous fluids with no appreciable change in her blood pressure. An electrocardiogram in this patient would most likely reveal which of the following findings?
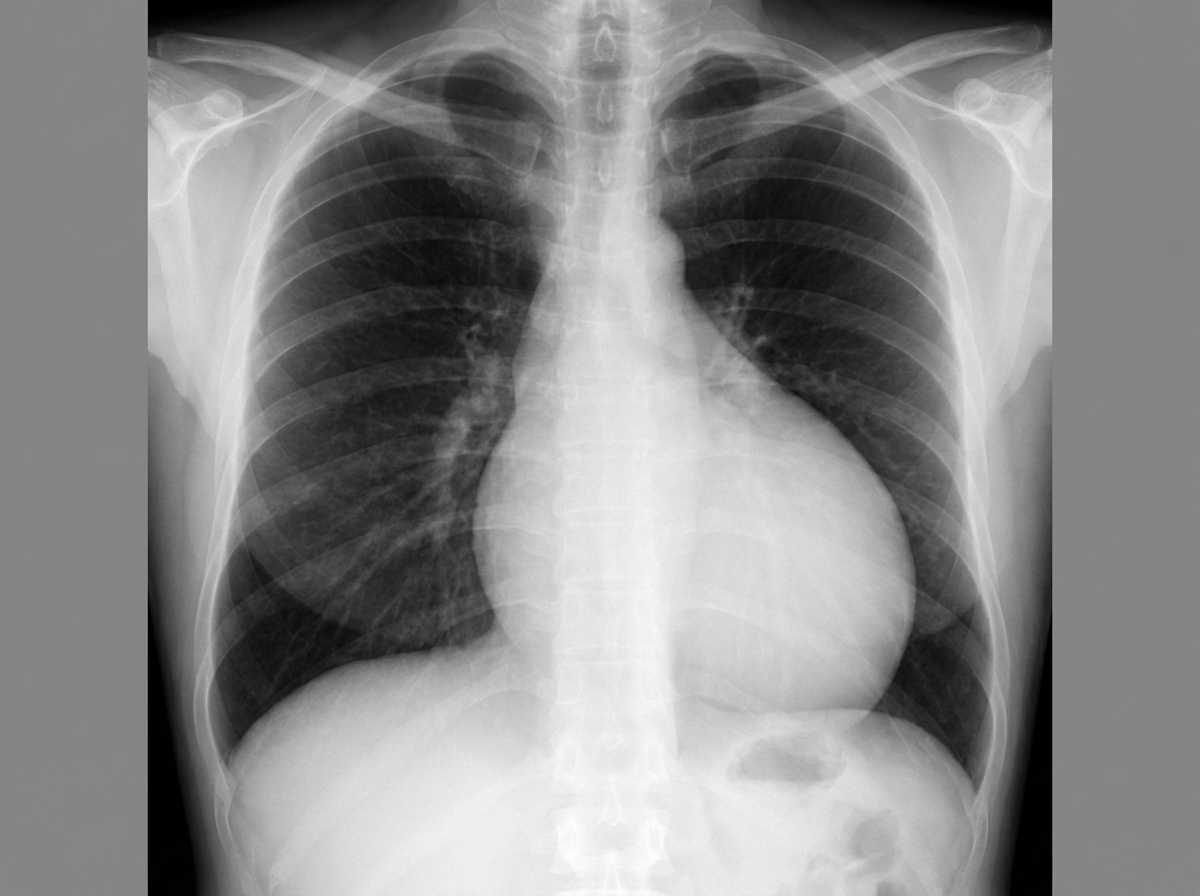
A 49-year-old man comes to the physician because of a 2-week history of increasing shortness of breath. He has also had chest pain that is exacerbated by deep inspiration. He has had recurrent episodes of pain in his fingers for the past 2 years. Two years ago, he was treated for a deep vein thrombosis. He has hypertension and anxiety. Current medications include enalapril, St John's wort, and ibuprofen. His temperature is 37°C (98.6°F), pulse is 110/min, respirations are 17/min, and blood pressure is 110/70 mm Hg. Examination shows pale conjunctiva. There is tenderness to palpation of the proximal interphalangeal and metacarpophalangeal joints of both hands. Heart sounds are distant. The lungs are clear to auscultation. Laboratory studies show: Hemoglobin 11.9 g/dL Leukocyte count 4200/mm3 Platelet count 330,000/mm3 Serum Na+ 136 mEq/L K+ 4.3 mEq/L Antinuclear antibodies 1: 320 Anti-Sm antibodies positive Anti-CCP antibodies negative An x-ray of the chest is shown. Which of the following is most likely to be seen on this patient's ECG?
A 50-year-old man presents the emergency department for intense chest pain, profuse sweating, and shortness of breath. The onset of these symptoms was 3 hours ago. The chest pain began after a heated discussion with a colleague at the community college where he is employed. Upon arrival, he is found conscious and responsive; the vital signs include a blood pressure of 130/80 mm Hg, a heart rate at 90/min, a respiratory rate at 20/min, and a body temperature of 36.4°C (97.5°F). His medical history is significant for hypertension diagnosed 7 years ago, which is well-controlled with a calcium channel blocker. The initial electrocardiogram (ECG) shows ST-segment depression in multiple consecutive leads, an elevated cardiac troponin T level, and normal kidney function. Which of the following would you expect to find in this patient?
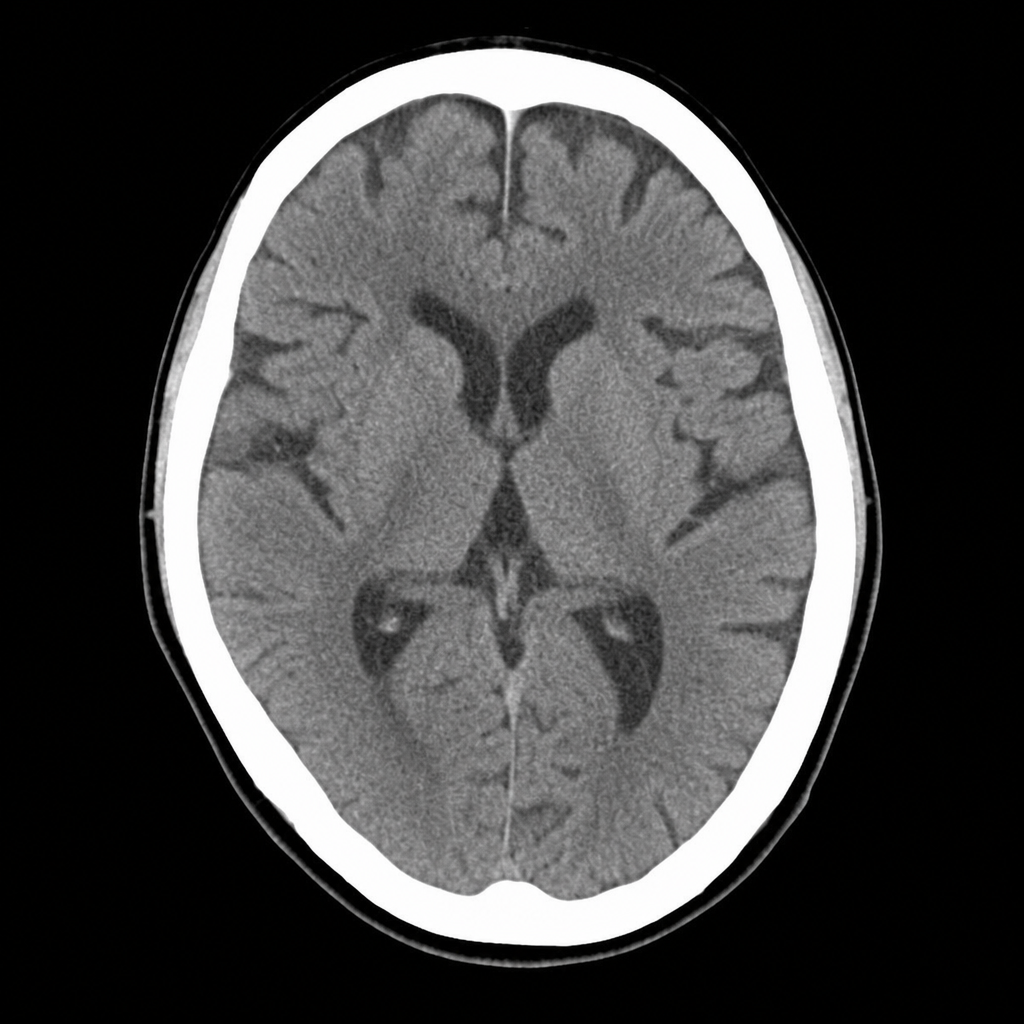
A 67-year-old man with hypertension and type 2 diabetes is brought to the ED by his wife, who noticed he developed sudden right-sided facial droop and slurred speech approximately 2 hours ago. On arrival, blood pressure is 188/104 mmHg, heart rate 82 bpm, oxygen saturation 97% on room air. Neurological examination reveals right facial weakness, dysarthria, and mild right arm drift. NIHSS score is 7. A non-contrast CT head is performed and shown above. No hemorrhage, early infarct signs, or mass lesion is identified. The patient takes metformin and lisinopril; no anticoagulants. Which of the following is the most appropriate immediate next step?
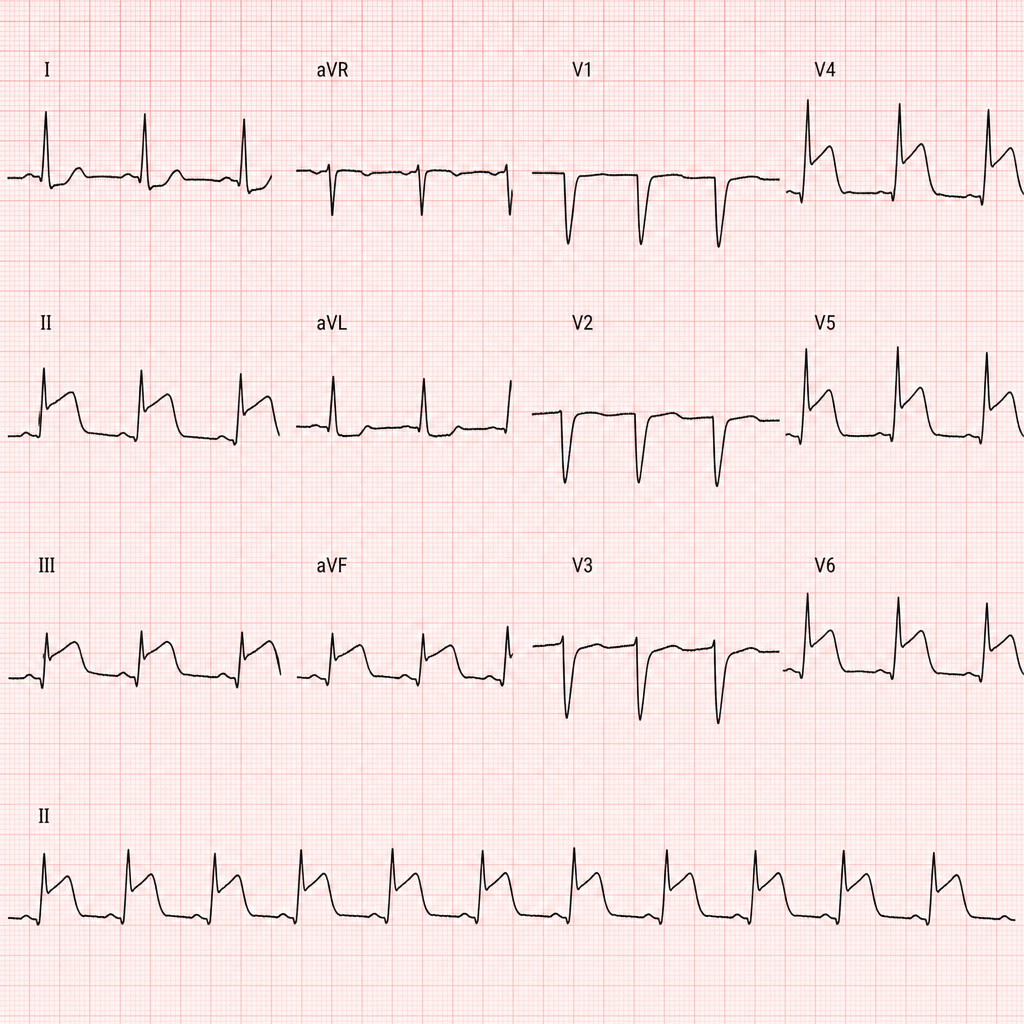
A 67-year-old man with hypertension and hyperlipidemia presents to the emergency department with 45 minutes of crushing substernal chest pain radiating to his left arm. He is diaphoretic and pale. Vital signs: BP 88/60 mmHg, HR 112 bpm, RR 20/min, SpO2 94% on room air. PCI is immediately available. An ECG is obtained and shown above. Two large-bore IVs are placed. Which of the following is the most appropriate immediate next step?
A 70-year-old man with diabetes, hypertension, and chronic kidney disease (eGFR 35 mL/min/1.73m²) presents with NSTEMI. Troponin is elevated at 8.5 ng/mL. ECG shows 2mm ST depression in V2-V5. GRACE score is 165 (high risk). He is hemodynamically stable. Cardiologist recommends early invasive strategy within 24 hours. Nephrologist is concerned about contrast-induced nephropathy potentially requiring dialysis. Patient is on metformin. Evaluate the management strategy integrating multiple specialist perspectives and evidence.
A 58-year-old woman with anterior STEMI underwent primary PCI with drug-eluting stent placement. Post-procedure echocardiogram shows left ventricular ejection fraction of 30% with apical akinesis. She is started on aspirin, ticagrelor, high-intensity statin, and ACE inhibitor. On hospital day 3, she develops atrial fibrillation with rapid ventricular response. CHA2DS2-VASc score is 4. Creatinine is normal. Evaluate the optimal antithrombotic strategy balancing ischemic and bleeding risk.
A 60-year-old man with inferoposterior STEMI presents to a rural hospital. The nearest PCI-capable facility is 3 hours away. He arrives 90 minutes after symptom onset. Blood pressure is 130/85 mmHg, heart rate 88/min, oxygen saturation 96% on room air. He has no contraindications to fibrinolysis. The transfer team can arrive in 30 minutes. Evaluate the evidence-based approach considering time metrics and available resources.
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app