
Biomarker interpretation — MCQs

A woman with coronary artery disease is starting to go for a walk. As she begins, her heart rate accelerates from a resting pulse of 60 bpm until it reaches a rate of 120 bpm, at which point she begins to feel a tightening in her chest. She stops walking to rest and the tightening resolves. This has been happening to her consistently for the last 6 months. Which of the following is a true statement?
A 66-year-old man comes to the emergency department because of a 1-day history of chest pain, palpitations, and dyspnea on exertion. He had a similar episode 3 days ago and was diagnosed with an inferior wall myocardial infarction. He was admitted and a percutaneous transluminal coronary angioplasty was successfully done that day. A fractional flow reserve test during the procedure showed complete resolution of the stenosis. Laboratory tests including serum glucose, lipids, and blood count were within normal limits. He was discharged the day after the procedure on a drug regimen of aspirin, simvastatin, and isosorbide dinitrate. At the time of discharge, he had no chest pain or dyspnea. Presently, his vitals are normal and ECG at rest shows new T-wave inversion. Which of the following is the most reliable test for rapidly establishing the diagnosis in this patient?
A 32-year-old man comes to the emergency department because of sharp chest pain for 3 days. The pain is retrosternal, 8 out of 10 in intensity, increases with respiration, and decreases while sitting upright and leaning forward. He has nausea and myalgia. He has not had fever or a cough. He has asthma and was treated for bronchitis 6 months ago with azithromycin. His mother has hypertension. He uses an over-the-counter inhaler. His temperature is 37.3°C (99.1°F), pulse is 110/min, and blood pressure is 130/84 mm Hg. Breath sounds are normal. Cardiac examination shows a high-pitched grating sound between S1 and S2. The remainder of the examination shows no abnormalities. Serum studies show: Urea nitrogen 16 mg/dl Glucose 103 mg/dL Creatinine 0.7 mg/dL Troponin I 0.230 ng/mL (N < 0.1 ng/mL) An ECG shows diffuse ST elevations in all leads. The patient is at increased risk for which of the following conditions?
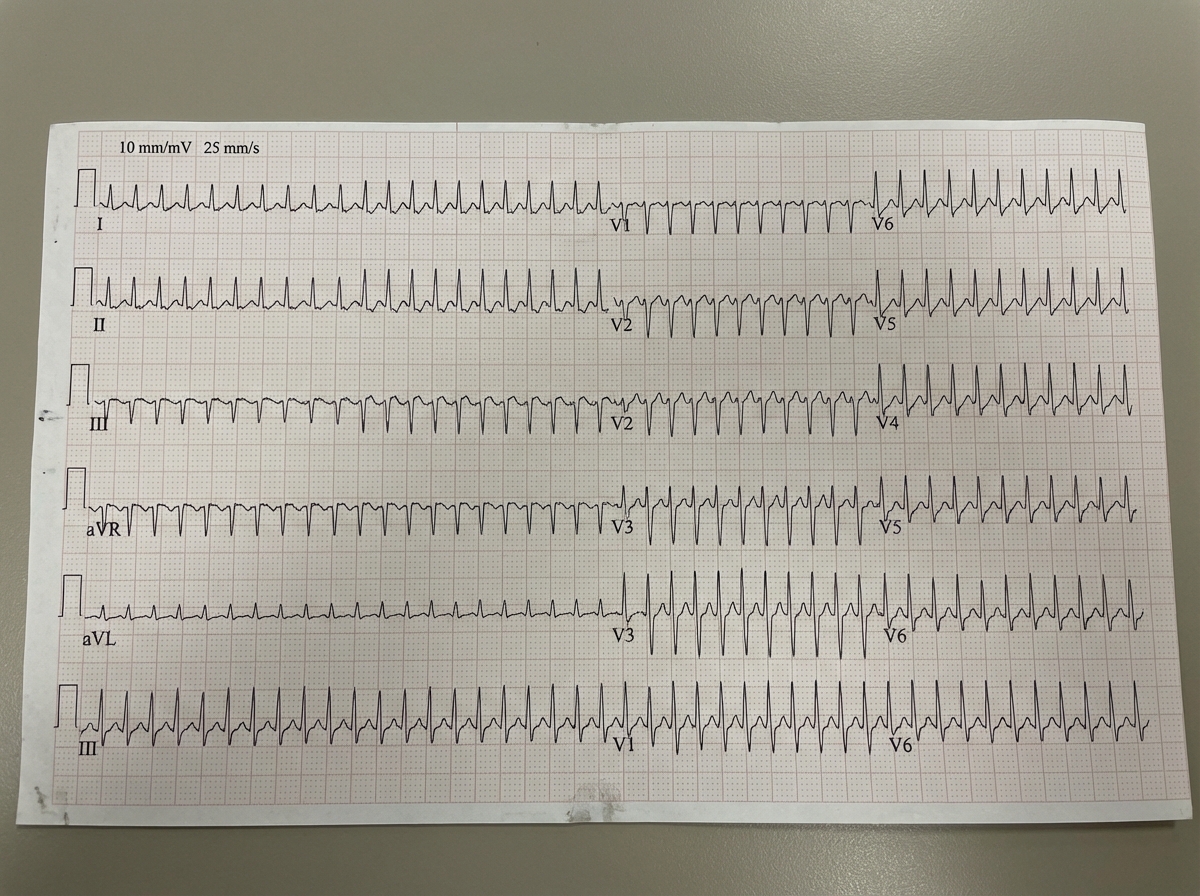
A 43-year-old man comes to the emergency room complaining of chest discomfort. He describes the feeling as "tightness," and also reports weakness and palpitations for the past hour. He denies shortness of breath, diaphoresis, or lightheadedness. He has no significant past medical history, and does not smoke, drink, or use illicit drugs. His father had a myocardial infarction at age 72. He is afebrile, heart rate is 125 bpm, and his blood pressure is 120/76. He is alert and oriented to person, place, and time. His electrocardiogram is shown below. Which of the following tests should be ordered in the initial work-up of this patient's condition?
A cardiologist is studying how a new virus that infects the heart affects the electrical conduction system of the cardiac myocytes. He decides to obtain electrocardiograms on patients with this disease in order to see how the wave patterns and durations change over time. While studying these records, he asks a medical student who is working with him to interpret the traces. Specifically, he asks her to identify the part that represents initial ventricular depolarization. Which of the following characteristics is most consistent with this feature of the electrocardiogram?
A 71-year-old man presents to the emergency department for shortness of breath. The patient was returning from a business trip to China, when he suddenly felt short of breath during the taxi ride home from the airport. The patient has a past medical history of poorly controlled diabetes mellitus and a 50 pack-year smoking history. The patient is non-compliant with his medications and is currently only taking ibuprofen. An initial ECG demonstrates sinus tachycardia. A chest radiograph is within normal limits. Laboratory values are notable for a creatinine of 2.4 mg/dL and a BUN of 32 mg/dL as compared to his baseline creatinine of 0.9 mg/dL. His temperature is 98.8°F (37.1°C), pulse is 122/min, blood pressure is 145/90 mmHg, respirations are 19/min, and oxygen saturation is 93% on room air. On physical exam, you note an older gentleman in distress. Cardiac exam is notable only for tachycardia. Pulmonary exam is notable for expiratory wheezes. Which of the following is the best confirmatory test for this patient?
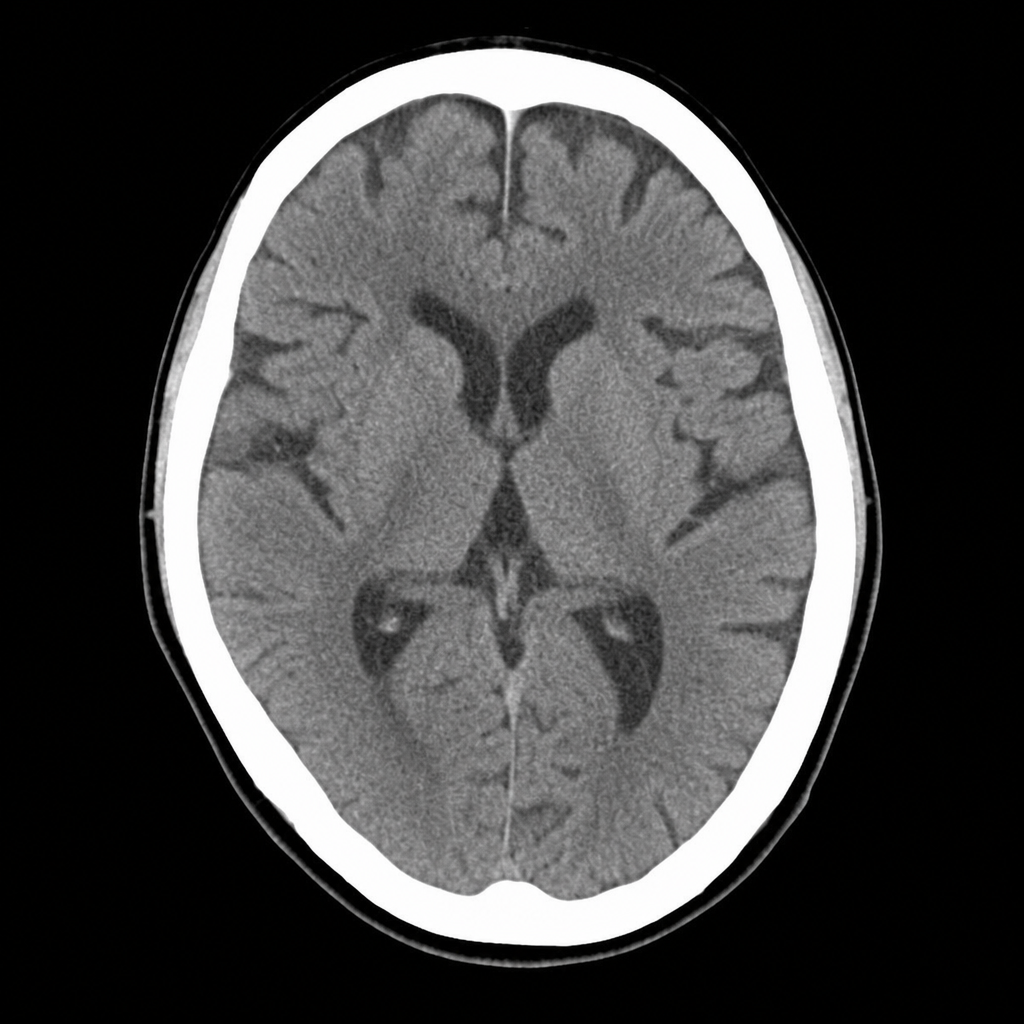
A 67-year-old man with hypertension and type 2 diabetes is brought to the ED by his wife, who noticed he developed sudden right-sided facial droop and slurred speech approximately 2 hours ago. On arrival, blood pressure is 188/104 mmHg, heart rate 82 bpm, oxygen saturation 97% on room air. Neurological examination reveals right facial weakness, dysarthria, and mild right arm drift. NIHSS score is 7. A non-contrast CT head is performed and shown above. No hemorrhage, early infarct signs, or mass lesion is identified. The patient takes metformin and lisinopril; no anticoagulants. Which of the following is the most appropriate immediate next step?
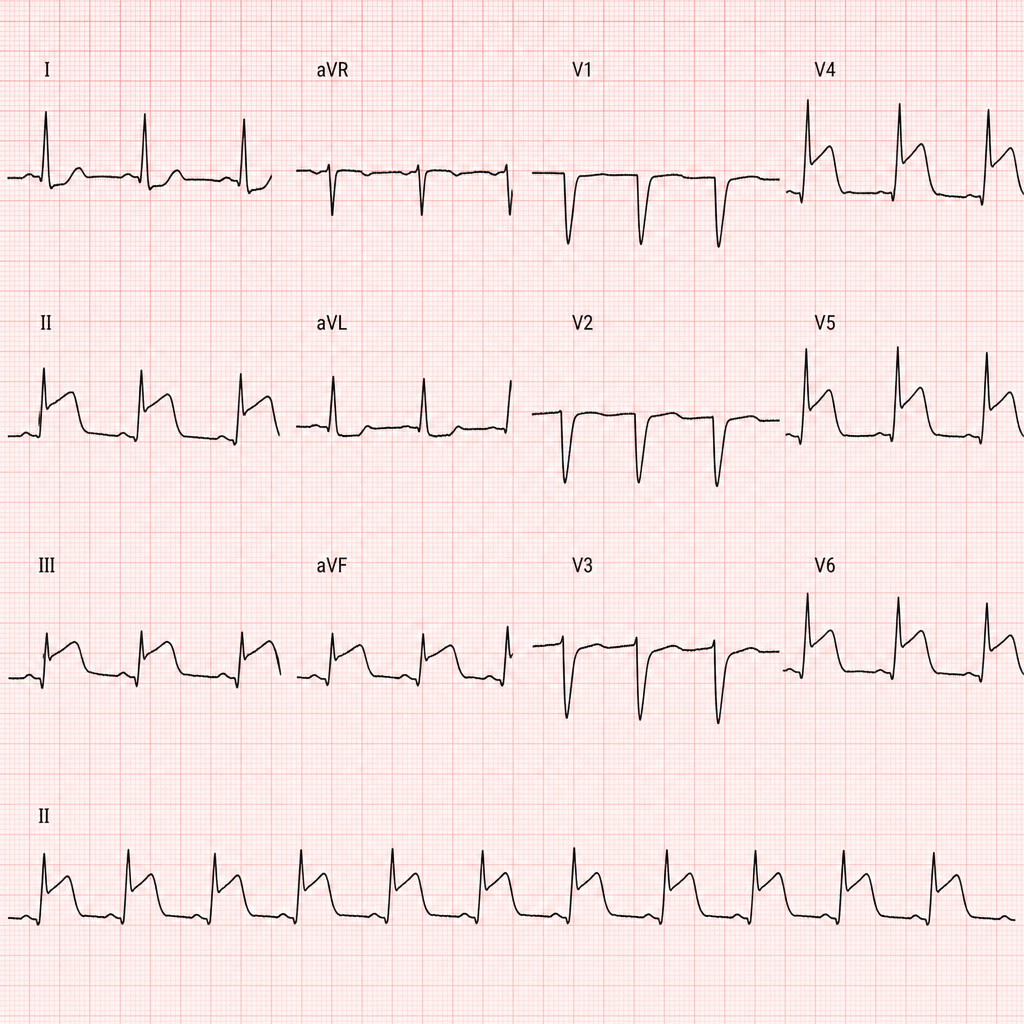
A 67-year-old man with hypertension and hyperlipidemia presents to the emergency department with 45 minutes of crushing substernal chest pain radiating to his left arm. He is diaphoretic and pale. Vital signs: BP 88/60 mmHg, HR 112 bpm, RR 20/min, SpO2 94% on room air. PCI is immediately available. An ECG is obtained and shown above. Two large-bore IVs are placed. Which of the following is the most appropriate immediate next step?
A 70-year-old man with diabetes, hypertension, and chronic kidney disease (eGFR 35 mL/min/1.73m²) presents with NSTEMI. Troponin is elevated at 8.5 ng/mL. ECG shows 2mm ST depression in V2-V5. GRACE score is 165 (high risk). He is hemodynamically stable. Cardiologist recommends early invasive strategy within 24 hours. Nephrologist is concerned about contrast-induced nephropathy potentially requiring dialysis. Patient is on metformin. Evaluate the management strategy integrating multiple specialist perspectives and evidence.
A 58-year-old woman with anterior STEMI underwent primary PCI with drug-eluting stent placement. Post-procedure echocardiogram shows left ventricular ejection fraction of 30% with apical akinesis. She is started on aspirin, ticagrelor, high-intensity statin, and ACE inhibitor. On hospital day 3, she develops atrial fibrillation with rapid ventricular response. CHA2DS2-VASc score is 4. Creatinine is normal. Evaluate the optimal antithrombotic strategy balancing ischemic and bleeding risk.
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app