
Arrhythmic complications management — MCQs

A 39-year-old woman is brought to the emergency department 30 minutes after her husband found her unconscious on the living room floor. She does not report having experienced light-headedness, nausea, sweating, or visual disturbance before losing consciousness. Three weeks ago, she was diagnosed with open-angle glaucoma and began treatment with an antiglaucoma drug in the form of eye drops. She last used the eye drops 1 hour ago. Examination shows pupils of normal size that are reactive to light. An ECG shows sinus bradycardia. This patient is most likely undergoing treatment with which of the following drugs?
A 62-year-old man is brought to the emergency department because of syncope. He reports sudden onset of palpitations followed by loss of consciousness while carrying his groceries to his car. He is unable to recall any further details and does not have any chest pain or dizziness. He has a history of hypertension, type 2 diabetes mellitus, gastroparesis, and osteoarthritis of the knees. Medications include lisinopril, metformin, and ondansetron as needed for nausea. He also takes methadone daily for chronic pain. Apart from an abrasion on his forehead, he appears well. His temperature is 37.2 °C (98.9 F), heart rate is 104/min and regular, and blood pressure is 135/70 mm Hg. While he is in the emergency department, he loses consciousness again. Telemetry shows polymorphic ventricular tachycardia with cyclic alteration of the QRS axis that spontaneously resolves after 30 seconds. Results of a complete blood count, serum electrolyte concentrations, and serum thyroid studies show no abnormalities. Cardiac enzymes are within normal limits. Which of the following is the most likely underlying cause of this patient's syncope?
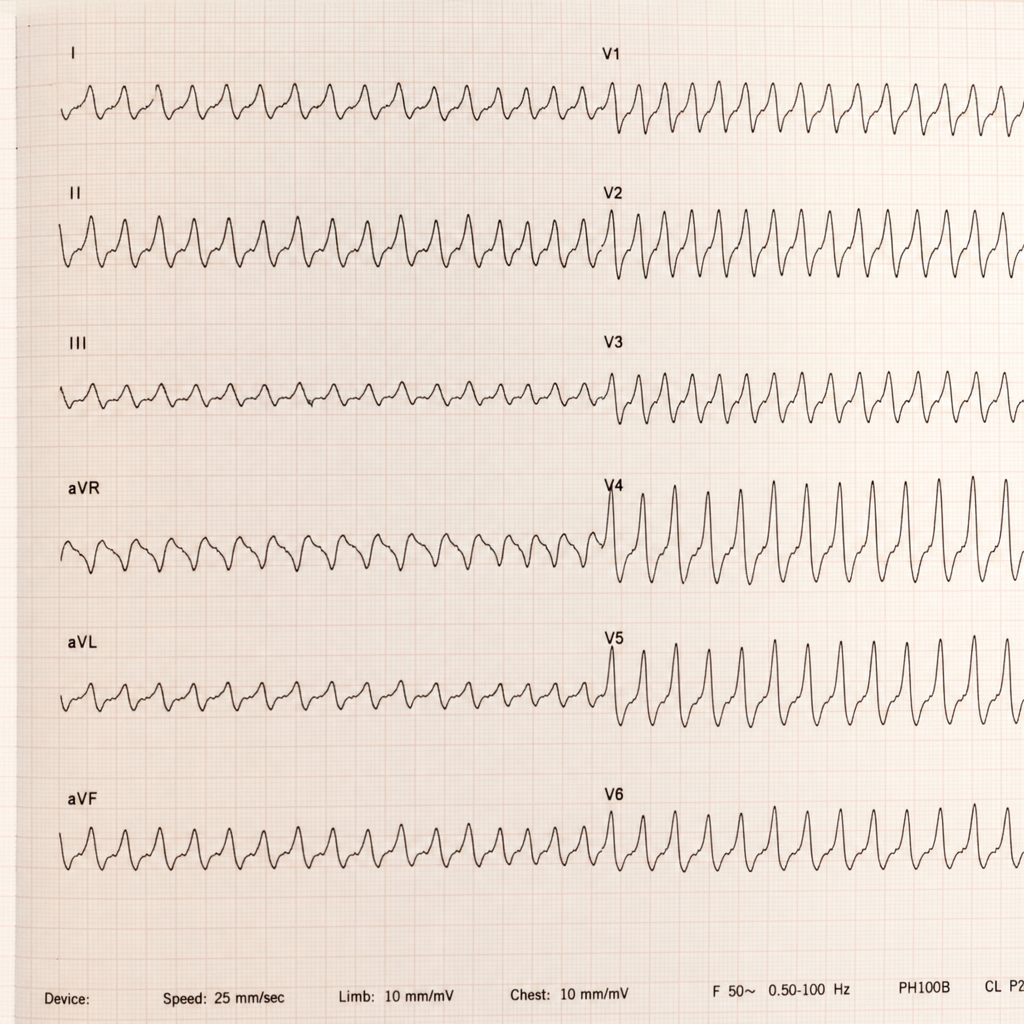
One week after an aortic valve replacement surgery, a 55-year-old man is brought to the emergency room 30 minutes after the onset of severe, sharp chest pain. He appears pale and dyspneic but is alert, oriented, and speaks in full sentences. His temperature is 38°C (100.4°F), pulse is 192/min and thready, respirations are 22/min, and blood pressure is 80/50 mm Hg. Faint rales can be heard in the lower lung fields on both sides on auscultation. There is a midline thoracotomy scar with mild reddening but without warmth or discharge. A portion of an ECG is shown. The pattern remains unchanged after 1 minute. Which of the following is the most appropriate intervention?
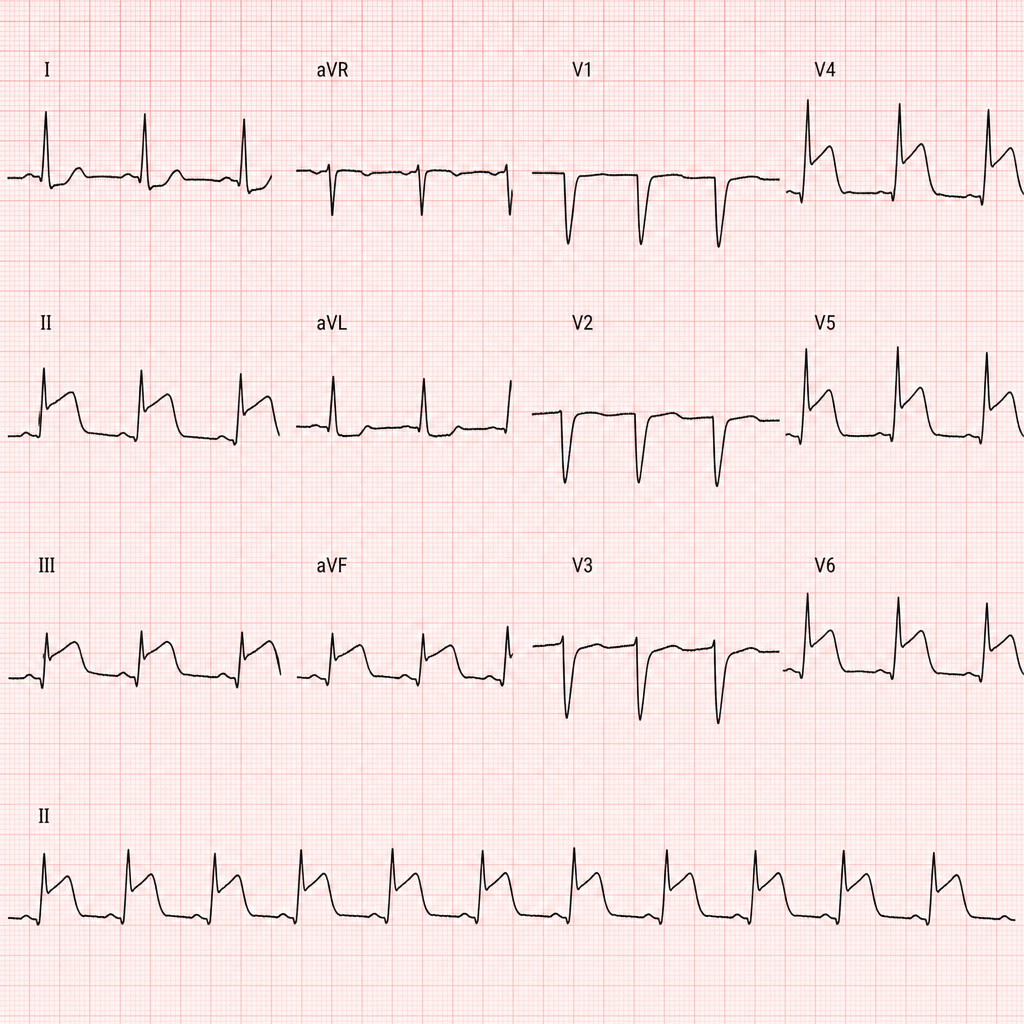
A 50-year-old woman presents to the emergency department with mild chest pressure that does not radiate to her left arm or jaw. These episodes have been ongoing several times over the last 24 hours. Her medical history is significant for diabetes mellitus type II and HTN for which she takes metformin and lisinopril. Her physical exam is significant for a middle aged woman appearing as stated age in moderate distress. Her heart and lung sounds are within normal limits. On laboratory examination, her troponin level is elevated, and her heart rate waivers around 47/min. Note this patient’s EKG in the exhibit. Which pacemaker site is likely in use in this patient?
A 63-year-old man with a history of hypertension and atrial fibrillation is brought into the emergency room and found to have a ventricular tachyarrhythmia. Ibutilide is discontinued and the patient is switched to another drug that also prolongs the QT interval but is associated with a decreased risk of torsades de pointes. Which drug was most likely administered in this patient?
A 65-year-old man with hypertension and paroxysmal atrial fibrillation presents to his cardiologist for follow-up after recently starting metoprolol for rate control. His EKG shows an atrial rate of 260/min with ventricular rate of 50/min on an irregular baseline. An echocardiogram from his previous visit revealed no evidence of hypokinesis or hypertrophy with functionally intact valves. The patient does not drink alcohol and had no evidence of liver dysfunction in prior studies. What is the best medication for rhythm control in this patient?
A 61-year-old man is brought to the emergency department by ambulance because of severe retrosternal chest pain and shortness of breath for 30 minutes. Paramedics report that an ECG recorded en route to the hospital showed ST-segment elevation in I, aVL, and the precordial leads. On arrival, the patient is unresponsive to painful stimuli. Examination shows neither respiration nor pulse. Despite appropriate lifesaving measures, he dies 10 minutes later. Which of the following is the most likely cause of death in this patient?
An 8-month-old boy is brought to the emergency department by his mother. She is concerned that her son has had intermittent periods of severe abdominal pain over the past several days that has been associated with emesis and "currant jelly" stool. Of note, the family lives in a rural part of the state, requiring a 2 hour drive to the nearest hospital. He currently appears to be in significant pain and has vomited twice in the past hour. On physical examination, a sausage-shaped mass is noted on palpation of the right upper quadrant of the abdomen. Ultrasound of the abdomen was consistent with a diagnosis of intussusception. An air-contrast barium enema was performed, which confirmed the diagnosis and also successfully reduced the intussusception. Which of the following is the next best step in the management of this patient?
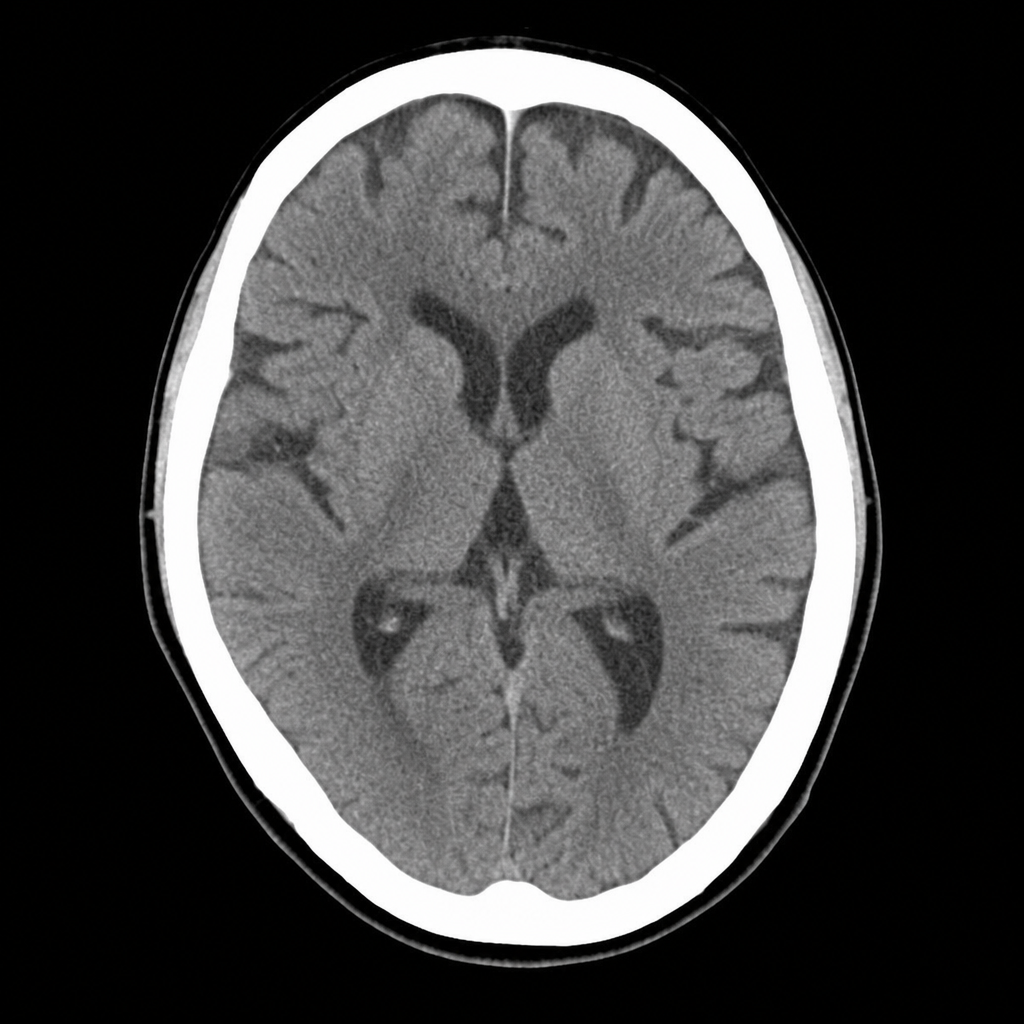
A 67-year-old man with hypertension and type 2 diabetes is brought to the ED by his wife, who noticed he developed sudden right-sided facial droop and slurred speech approximately 2 hours ago. On arrival, blood pressure is 188/104 mmHg, heart rate 82 bpm, oxygen saturation 97% on room air. Neurological examination reveals right facial weakness, dysarthria, and mild right arm drift. NIHSS score is 7. A non-contrast CT head is performed and shown above. No hemorrhage, early infarct signs, or mass lesion is identified. The patient takes metformin and lisinopril; no anticoagulants. Which of the following is the most appropriate immediate next step?
A 67-year-old man with hypertension and hyperlipidemia presents to the emergency department with 45 minutes of crushing substernal chest pain radiating to his left arm. He is diaphoretic and pale. Vital signs: BP 88/60 mmHg, HR 112 bpm, RR 20/min, SpO2 94% on room air. PCI is immediately available. An ECG is obtained and shown above. Two large-bore IVs are placed. Which of the following is the most appropriate immediate next step?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app