
Antiplatelet management — MCQs

You are conducting a study comparing the efficacy of two different statin medications. Two groups are placed on different statin medications, statin A and statin B. Baseline LDL levels are drawn for each group and are subsequently measured every 3 months for 1 year. Average baseline LDL levels for each group were identical. The group receiving statin A exhibited an 11 mg/dL greater reduction in LDL in comparison to the statin B group. Your statistical analysis reports a p-value of 0.052. Which of the following best describes the meaning of this p-value?
A 66-year-old woman presents to the emergency department complaining of palpitations. She says that she has been experiencing palpitations and lightheadedness for the past 6 months, but before this morning the episodes usually resolved on their own. The patient's medical history is significant for a transient ischemia attack 2 months ago, hypertension, and diabetes. She takes aspirin, metformin, and lisinopril. She states her grandfather died of a stroke, and her mom has a "blood disorder." An electrocardiogram is obtained that shows an irregularly irregular rhythm with rapid ventricular response, consistent with atrial fibrillation. She is given intravenous metoprolol, which resolves her symptoms. In addition to starting a beta-blocker for long-term management, the patient meets criteria for anticoagulation. Both unfractionated heparin and warfarin are started. Five days later, the patient begins complaining of pain and swelling of her left lower extremity. A Doppler ultrasound reveals thrombosis in her left popliteal and tibial veins. A complete blood count is obtained that shows a decrease in platelet count from 245,000/mm^3 to 90,000/mm^3. Coagulation studies are shown below: Prothrombin time (PT): 15 seconds Partial thromboplastin time (PTT): 37 seconds Bleeding time: 14 minutes Which of the following is the most likely diagnosis?
A 54-year-old man comes to the physician for a follow-up examination. One week ago, he was treated in the emergency department for chest pain, palpitations, and dyspnea. As part of his regimen, he was started on a medication that irreversibly inhibits the synthesis of thromboxane A2 and prostaglandins. Which of the following is the most likely adverse effect of this medication?
A primary care physician who focuses on treating elderly patients is researching recommendations for secondary prevention. She is particularly interested in recommendations regarding aspirin, as she has several patients who ask her if they should take it. Of the following, which patient should be started on lifelong aspirin as monotherapy for secondary prevention of atherosclerotic cardiovascular disease?
A 3-year-old male is evaluated for frequent nose bleeds. Physical examination shows diffuse petechiae on the patient's distal extremities. Peripheral blood smear shows an absence of platelet clumping. An ELISA binding assay reveals that platelet surfaces are deficient in GpIIb/IIIa receptors. Which of the following drugs pharmacologically mimics this condition?
A 49-year-old man with a past medical history of hypertension on amlodipine presents to your office to discuss ways to lessen his risk of complications from heart disease. After a long discussion, he decides to significantly decrease his intake of trans fats in an attempt to lower his risk of coronary artery disease. Which type of prevention is this patient initiating?
A 70-year-old male presents for an annual exam. His past medical history is notable for shortness of breath when he sleeps, and upon exertion. Recently he has experienced dyspnea and lower extremity edema that seems to be worsening. Both of these symptoms have resolved since he was started on several medications and instructed to weigh himself daily. Which of the following is most likely a component of his medical management?
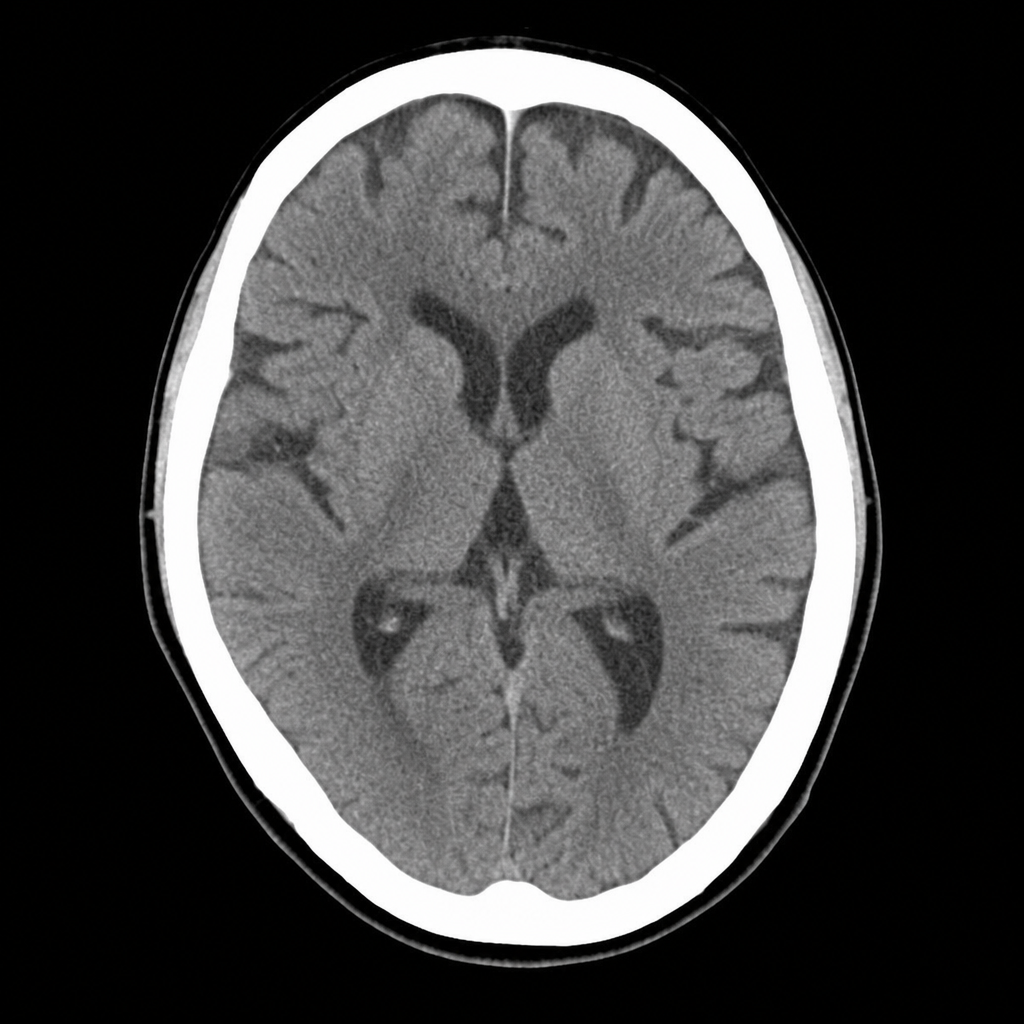
A 67-year-old man with hypertension and type 2 diabetes is brought to the ED by his wife, who noticed he developed sudden right-sided facial droop and slurred speech approximately 2 hours ago. On arrival, blood pressure is 188/104 mmHg, heart rate 82 bpm, oxygen saturation 97% on room air. Neurological examination reveals right facial weakness, dysarthria, and mild right arm drift. NIHSS score is 7. A non-contrast CT head is performed and shown above. No hemorrhage, early infarct signs, or mass lesion is identified. The patient takes metformin and lisinopril; no anticoagulants. Which of the following is the most appropriate immediate next step?
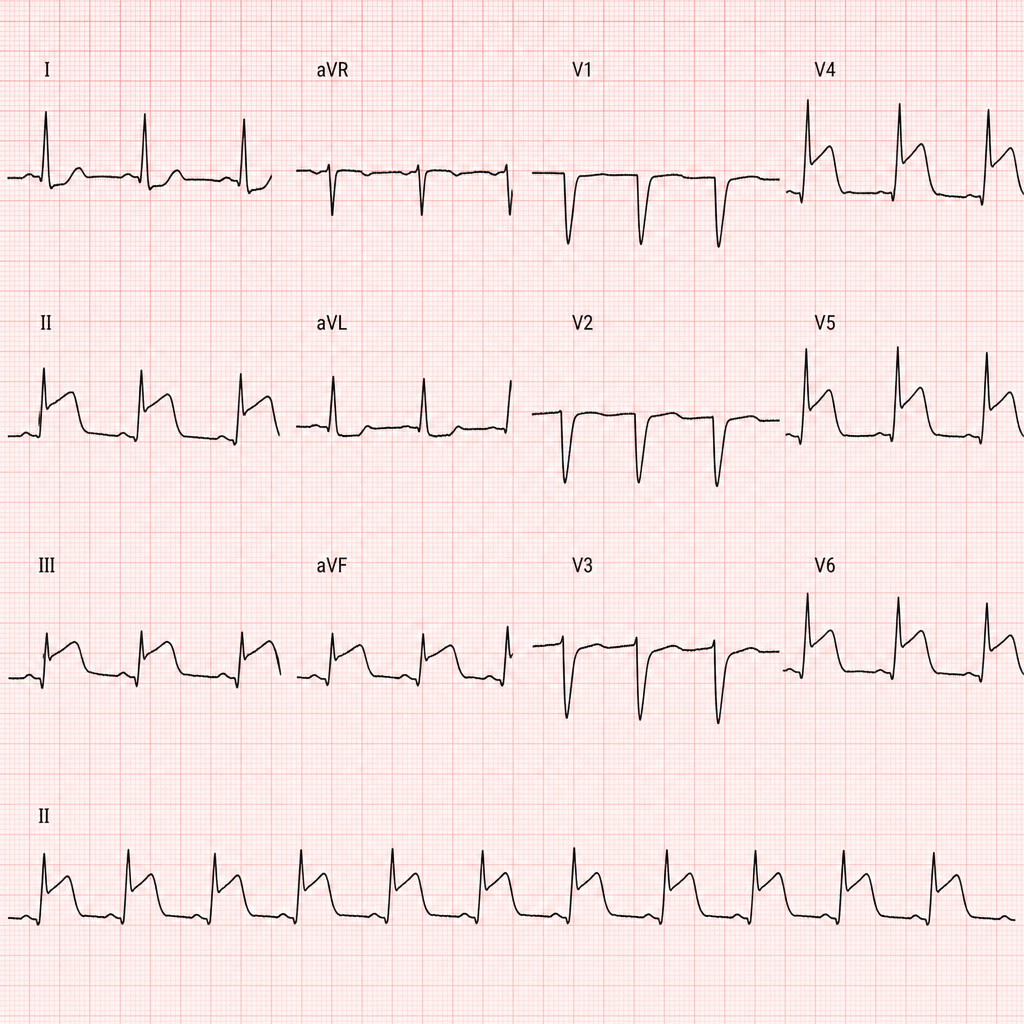
A 67-year-old man with hypertension and hyperlipidemia presents to the emergency department with 45 minutes of crushing substernal chest pain radiating to his left arm. He is diaphoretic and pale. Vital signs: BP 88/60 mmHg, HR 112 bpm, RR 20/min, SpO2 94% on room air. PCI is immediately available. An ECG is obtained and shown above. Two large-bore IVs are placed. Which of the following is the most appropriate immediate next step?
A 70-year-old man with diabetes, hypertension, and chronic kidney disease (eGFR 35 mL/min/1.73m²) presents with NSTEMI. Troponin is elevated at 8.5 ng/mL. ECG shows 2mm ST depression in V2-V5. GRACE score is 165 (high risk). He is hemodynamically stable. Cardiologist recommends early invasive strategy within 24 hours. Nephrologist is concerned about contrast-induced nephropathy potentially requiring dialysis. Patient is on metformin. Evaluate the management strategy integrating multiple specialist perspectives and evidence.
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app