
MI — MCQs

On this page
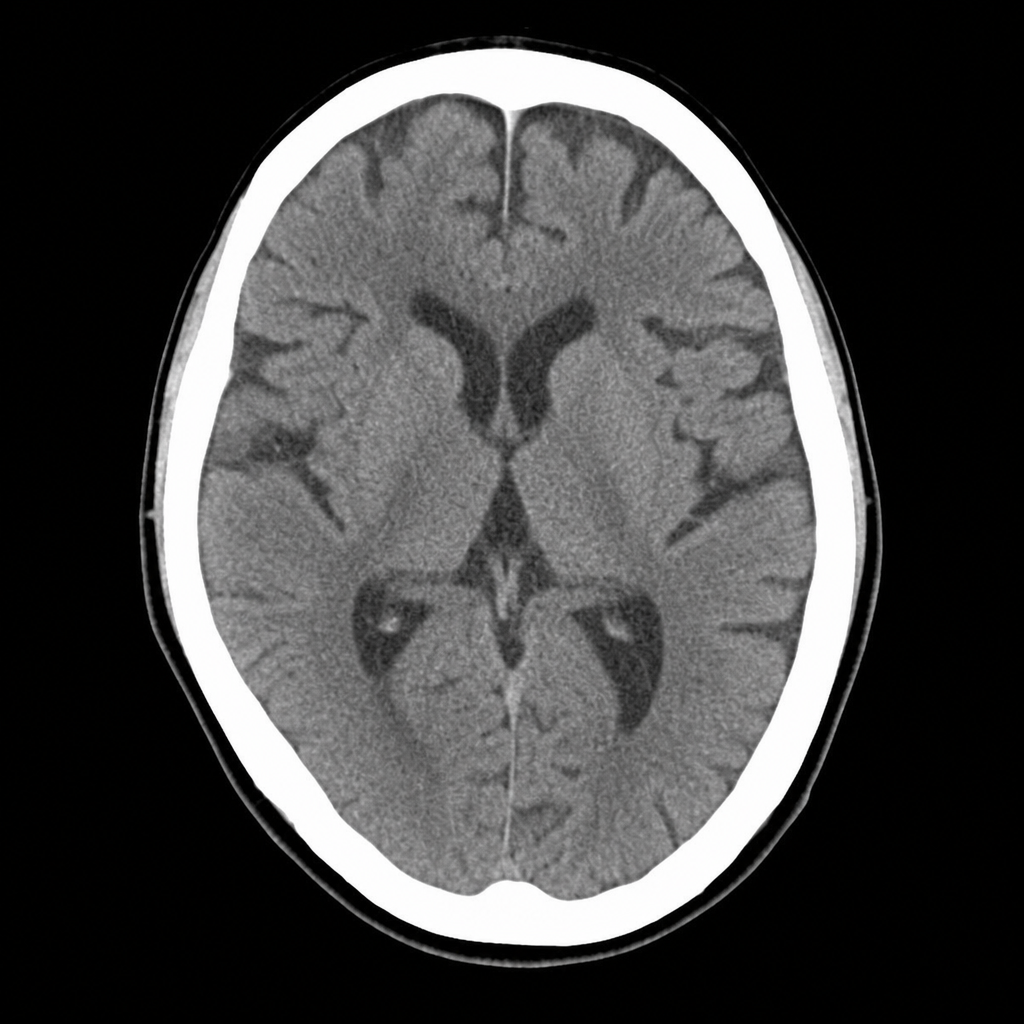
A 67-year-old man with hypertension and type 2 diabetes is brought to the ED by his wife, who noticed he developed sudden right-sided facial droop and slurred speech approximately 2 hours ago. On arrival, blood pressure is 188/104 mmHg, heart rate 82 bpm, oxygen saturation 97% on room air. Neurological examination reveals right facial weakness, dysarthria, and mild right arm drift. NIHSS score is 7. A non-contrast CT head is performed and shown above. No hemorrhage, early infarct signs, or mass lesion is identified. The patient takes metformin and lisinopril; no anticoagulants. Which of the following is the most appropriate immediate next step?
Practice by Chapter
Initial assessment and triage
Practice Questions
ECG interpretation in MI
Practice Questions
Biomarker interpretation
Practice Questions
STEMI management algorithm
Practice Questions
NSTEMI management algorithm
Practice Questions
Reperfusion strategies (fibrinolysis vs PCI)
Practice Questions
Antithrombotic therapies
Practice Questions
Antiplatelet management
Practice Questions
Beta-blockers, ACE-I/ARBs, statins
Practice Questions
Mechanical complications management
Practice Questions
Arrhythmic complications management
Practice Questions
Cardiogenic shock management
Practice Questions
Post-MI secondary prevention
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app