
Rheumatology (autoimmune diseases, arthritis) — MCQs

On this page
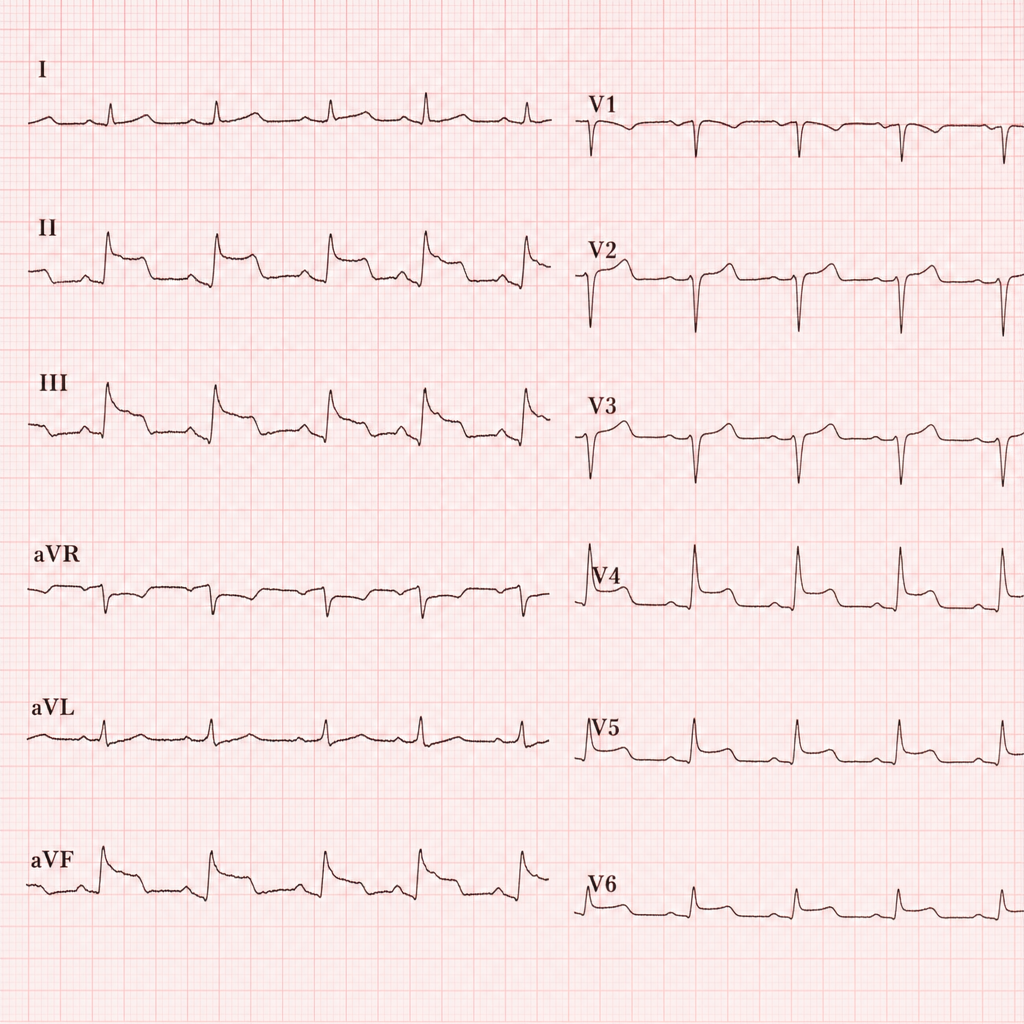
A 68-year-old woman with a history of type 2 diabetes and hypertension presents to the emergency department with 3 hours of epigastric discomfort, nausea, and diaphoresis. She denies chest pain. Her blood pressure is 148/92 mmHg, heart rate is 96 bpm, and oxygen saturation is 97% on room air. An ECG is obtained showing 2–3 mm ST-segment elevation in leads II, III, and aVF with reciprocal ST-segment depression in leads I and aVL. Physical examination reveals mild epigastric tenderness without guarding. Troponin I is pending. Which of the following is the most appropriate immediate next step in management?
A 26-year-old woman presents with 8 weeks of symmetric polyarthritis affecting hands, wrists, and feet with 90 minutes of morning stiffness. RF negative, anti-CCP negative, ANA 1:160 (homogeneous), ESR 45 mm/hr. She has no rash, oral ulcers, or systemic symptoms. Radiographs show soft tissue swelling without erosions. She desires pregnancy within the year. Apply the most appropriate initial management considering her reproductive plans.
A 58-year-old woman presents with bilateral shoulder and hip girdle pain and stiffness for 6 weeks. She has difficulty rising from a chair and combing her hair. ESR 72 mm/hr, CRP 6.8 mg/dL, CK normal, RF negative, ANA negative. She responds dramatically to prednisone 15 mg daily within 48 hours. Three months later, while tapering to 7.5 mg daily, she develops new-onset headache and scalp tenderness. ESR is now 85 mm/hr. Temporal artery biopsy shows non-specific inflammation. Apply the appropriate management modification.
A 50-year-old man with psoriatic arthritis on methotrexate 20 mg weekly presents with worsening polyarthritis despite 6 months of therapy. He has active dactylitis, enthesitis at Achilles insertion, and progressive erosive changes on hand radiographs. Liver enzymes are normal, creatinine 1.0 mg/dL. He also has moderate plaque psoriasis covering 15% body surface area. His insurance requires step therapy and has denied biologic coverage. Evaluate the most appropriate advocacy and management approach.
A 42-year-old man with ankylosing spondylitis on adalimumab for 2 years presents with progressive dyspnea. He is a non-smoker. PFTs show FVC 72% predicted, FEV1 78% predicted, FEV1/FVC 0.88, TLC 65% predicted. CT chest shows upper lobe fibrosis and cavitation. He also has new-onset heart block on ECG. Sputum cultures are negative for acid-fast bacilli after 3 samples. Analyze the most likely cause of his pulmonary and cardiac findings.
A 35-year-old woman with SLE on hydroxychloroquine and prednisone 10 mg daily presents at 10 weeks gestation with increased lupus disease activity including new-onset proteinuria (2 g/24h), arthritis, and rash. Labs show anti-dsDNA positive, low C3/C4, creatinine 1.2 mg/dL (baseline 0.8). Renal biopsy shows class III lupus nephritis. She desires to continue the pregnancy. Evaluate the optimal management strategy balancing maternal disease control and fetal safety.
A 68-year-old man presents with sudden onset severe headache, jaw claudication, and vision changes in his right eye. ESR is 98 mm/hr, CRP 8.5 mg/dL. Temporal artery is tender and non-pulsatile. Ophthalmology confirms anterior ischemic optic neuropathy. Temporal artery biopsy is scheduled for 3 days later. Apply the most appropriate immediate management.
A 45-year-old woman with systemic sclerosis (limited cutaneous type) presents with progressive dyspnea on exertion. She has had Raynaud's phenomenon for 15 years and skin thickening limited to hands and face. Pulmonary function tests show FVC 68% predicted, DLCO 52% predicted with preserved FEV1/FVC ratio. High-resolution CT chest shows ground-glass opacities and reticular changes in bilateral lower lobes. Right heart catheterization shows mean pulmonary artery pressure of 32 mmHg, pulmonary capillary wedge pressure 10 mmHg. Analyze the primary pulmonary complication and appropriate management.
A 55-year-old man with a 10-year history of rheumatoid arthritis on methotrexate and etanercept presents with sudden onset of right eye pain, redness, and photophobia. Visual acuity is decreased. Slit lamp examination reveals anterior chamber cells and flare. The patient also reports lower back stiffness worse in the morning that has developed over the past year. ESR is 42 mm/hr. HLA-B27 testing is positive. Analyze the most likely diagnosis and pathophysiologic relationship.
A 28-year-old African American woman presents with facial rash, arthralgia, and fatigue for 3 months. She has photosensitivity and oral ulcers. Labs show ANA 1:640 (speckled pattern), anti-dsDNA positive, anti-Smith antibody positive, complement C3 45 mg/dL (low), C4 8 mg/dL (low), WBC 3,200/μL, hemoglobin 10.2 g/dL, platelets 95,000/μL, creatinine 1.8 mg/dL. Urinalysis shows 3+ protein, RBC casts, and dysmorphic RBCs. Apply the most appropriate next diagnostic step.
Practice by Chapter
Rheumatoid arthritis
Practice Questions
Seronegative spondyloarthropathies
Practice Questions
Systemic lupus erythematosus
Practice Questions
Systemic sclerosis (scleroderma)
Practice Questions
Inflammatory myopathies
Practice Questions
Sjögren's syndrome
Practice Questions
Vasculitides classification
Practice Questions
Large vessel vasculitis
Practice Questions
Medium vessel vasculitis
Practice Questions
Small vessel vasculitis
Practice Questions
Crystal arthropathies (gout, pseudogout)
Practice Questions
Osteoarthritis
Practice Questions
DMARDs and biologic therapies
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app