
Sleep-disordered breathing — MCQs

A 63-year-old man presents to his primary care physician complaining of excessive daytime sleepiness. He explains that this problem has worsened slowly over the past few years but is now interfering with his ability to play with his grandchildren. He worked previously as an overnight train conductor, but he has been retired for the past 3 years. He sleeps approximately 8-9 hours per night and believes his sleep quality is good; however, his wife notes that he often snores loudly during sleep. He has never experienced muscle weakness or hallucinations. He has also been experiencing headaches in the morning and endorses a depressed mood. His physical exam is most notable for his large body habitus, with a BMI of 34. What is the best description of the underlying mechanism for this patient's excessive daytime sleepiness?
A 54-year-old man comes to the physician because of excessive daytime sleepiness for 5 months. He wakes up frequently at night, and his wife says his snoring has become louder. He is 180 cm (5 ft 10 in) tall and weighs 104 kg (230 lb); his BMI is 33 kg/m2. His pulse is 80/min and his respiratory rate is 11/min. His jugular venous pressure is 7 cm H2O. He has 2+ pitting edema of the lower legs and ankles. Arterial blood gas analysis on room air shows a pH of 7.42 and a PCO2 of 41 mm Hg. An x-ray of the chest shows normal findings. Which of the following is the most likely underlying cause of this patient's condition?
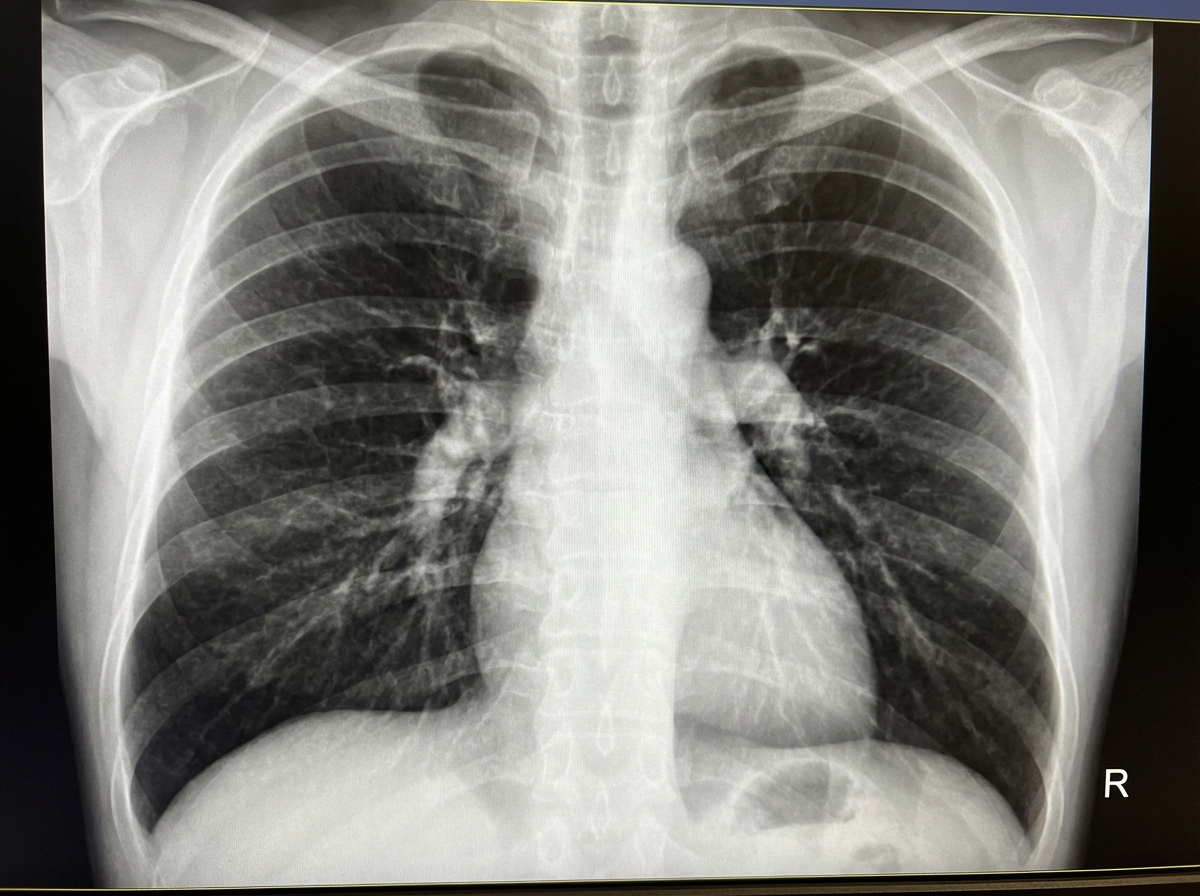
A 68-year-old man presents with shortness of breath, particularly when walking up stairs and when lying down to go to sleep at night. He also complains of a chronic cough and states that he now uses 2 extra pillows at night. The patient has a history of type 2 diabetes that is well-managed with metformin. He also takes Prozac for a long-standing history of depression. The patient has a 60-pack-year smoking history. He also has a history significant for alcohol abuse, but he quit cold turkey 15 years ago when his brother was killed in a drunk driving accident. Both he and his brother were adopted, and he does not know other members of his biological family. Despite repeated efforts of patient counseling, the patient is not interested in quitting smoking. The physical exam is significant for an obese male using accessory muscles of respiration. The vital signs include: temperature 36.8°C (98.2°F), heart rate 95/min, respiratory rate 16/min, and blood pressure 130/85 mm Hg. The oxygen saturation is 90% on room air. Additional physical exam findings include cyanotic lips, peripheral edema, hepatomegaly, and ascites. The cardiovascular exam is significant for an S3 heart sound and elevated JVP. The pulmonary exam is significant for expiratory wheezing, diffuse rhonchi, and hyperresonance on percussion. The laboratory test results are as follows: BUN 15 mg/dL pCO2 60 mm Hg Bicarbonate (HCO3) 32 mmol/L Creatinine 0.8 mg/dL Glucose 95 mg/dL Serum chloride 103 mmol/L Serum potassium 3.9 mEq/L Serum sodium 140 mEq/L Total calcium 2.3 mmol/L Hemoglobin 26 g/dL Bilirubin total 0.9 mg/dL Bilirubin indirect 0.4 mg/dL Iron 100 Ferritin 70 TIBC 300 The posterior-anterior chest X-ray is shown in the image. Which of the following interventions is indicated for decreasing the mortality of this patient?
A 65-year-old male with multiple comorbidities presents to your office complaining of difficulty falling asleep. Specifically, he says he has been having trouble breathing while lying flat very shortly after going to bed. He notes it only gets better when he adds several pillows, but that sitting up straight is an uncomfortable position for him in which to fall asleep. What is the most likely etiology of this man's sleeping troubles?
A 56-year-old man presents to the physician for the evaluation of excess snoring over the past year. He has no history of a serious illness and takes no medications. He does not smoke. His blood pressure is 155/95 mm Hg. BMI is 49 kg/m2. Oropharyngeal examination shows an enlarged uvula. Examination of the nasal cavity shows no septal deviation or polyps. Examination of the lungs and heart shows no abnormalities. Polysomnography shows an apnea-hypopnea index of 2 episodes/h with a PCO2 of 51 mm Hg during REM sleep. Arterial blood gas analysis in room air shows: pH 7.33 PCO2 50 mm Hg PO2 92 mm Hg HCO3− 26 mEq/L Which of the following best explains these findings?
A 15-year-old boy is brought to the physician with excessive daytime sleepiness over the past year. His parents are concerned with his below-average school performance over the last 3 months. He goes to bed around midnight and wakes up at 7 am on school days, but sleeps in late on weekends. He exercises regularly after school. He usually has a light snack an hour before bed. He does not snore or have awakenings during sleep. He has no history of a serious illness and takes no medications. The boy was born at 39 weeks gestation via spontaneous vaginal delivery. He is up to date on all vaccines and is meeting all developmental milestones. He does not smoke or drink alcohol. There is no history of a similar problem in the family. His vital signs are within normal limits. His BMI is 22 kg/m2. Physical examination shows no abnormal findings. Which of the following is the most appropriate recommendation at this time?
A 37-year-old man presents to his primary care physician because he has been experiencing episodes where he wakes up at night gasping for breath. His past medical history is significant for morbid obesity as well as hypertension for which he takes lisinopril. He is diagnosed with sleep apnea and prescribed a continuous positive airway pressure apparatus. In addition, the physician discusses making lifestyle and behavioral changes such as dietary modifications and exercise. The patient agrees to attempt these behavioral changes. Which of the following is most likely to result in improving patient adherence to this plan?
A 49-year-old woman comes to the physician because of a 4-month history of a dry cough and shortness of breath on exertion. She also reports recurrent episodes of pain, stiffness, and swelling in her wrist and her left knee over the past 6 months. She had two miscarriages at age 24 and 28. Physical examination shows pallor, ulcerations on the palate, and annular hyperpigmented plaques on the arms and neck. Fine inspiratory crackles are heard over bilateral lower lung fields on auscultation. Which of the following additional findings is most likely in this patient?
A 35-year-old woman who was recently ill with an upper respiratory infection presents to the emergency department with weakness in her lower limbs and difficulty breathing. Her symptoms began with a burning sensation in her toes along with numbness. She claims that the weakness has been getting worse over the last few days and now involving her arms and face. Currently, she is unable to get up from the chair without some assistance. Her temperature is 37.0°C (98.6°F), the blood pressure is 145/89 mm Hg, the heart rate is 99/min, the respiratory rate is 12/min, and the oxygen saturation is 95% on room air. On physical examination, she has diminished breath sounds on auscultation of bilateral lung fields with noticeably poor inspiratory effort. Palpation of the lower abdomen reveals a palpable bladder. Strength is 3 out of 5 symmetrically in the lower extremities bilaterally. The sensation is intact. What is the most likely diagnosis?
A 47-year-old patient returns to his primary care physician after starting aspirin two weeks ago for primary prevention of coronary artery disease. He complains that he wakes up short of breath in the middle of the night and has had coughing "attacks" three times. After discontinuing aspirin, what medication is most appropriate for prevention of similar symptoms in this patient?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app