
Pulmonary function testing interpretation — MCQs

A 60-year-old woman presents to the clinic with a 3-month history of shortness of breath that worsens on exertion. She also complains of chronic cough that has lasted for 10 years. Her symptoms are worsened even with light activities like climbing up a flight of stairs. She denies any weight loss, lightheadedness, or fever. Her medical history is significant for hypertension, for which she takes amlodipine daily. She has a 70-pack-year history of cigarette smoking and drinks 3–4 alcoholic beverages per week. Her blood pressure today is 128/84 mm Hg. A chest X-ray shows flattening of the diaphragm bilaterally. Physical examination is notable for coarse wheezing bilaterally. Which of the following is likely to be seen with pulmonary function testing?
A 62-year-old man presents to the emergency department for evaluation of a 2-year history of increasing shortness of breath. He also has an occasional nonproductive cough. The symptoms get worse with exertion. The medical history is significant for hypertension and he takes chlorthalidone. He is a smoker with a 40-pack-year smoking history. On physical examination, the patient is afebrile; the vital signs include: blood pressure 125/78 mm Hg, pulse 90/min, and respiratory rate 18/min. The body mass index (BMI) is 31 kg/m2. The oxygen saturation is 94% at rest on room air. A pulmonary examination reveals decreased breath sounds bilaterally, but is otherwise normal with no wheezes or crackles. The remainder of the examination is unremarkable. A chest radiograph shows hyperinflation of both lungs with mildly increased lung markings, but no focal findings. Based on this clinical presentation, which of the following is most likely?
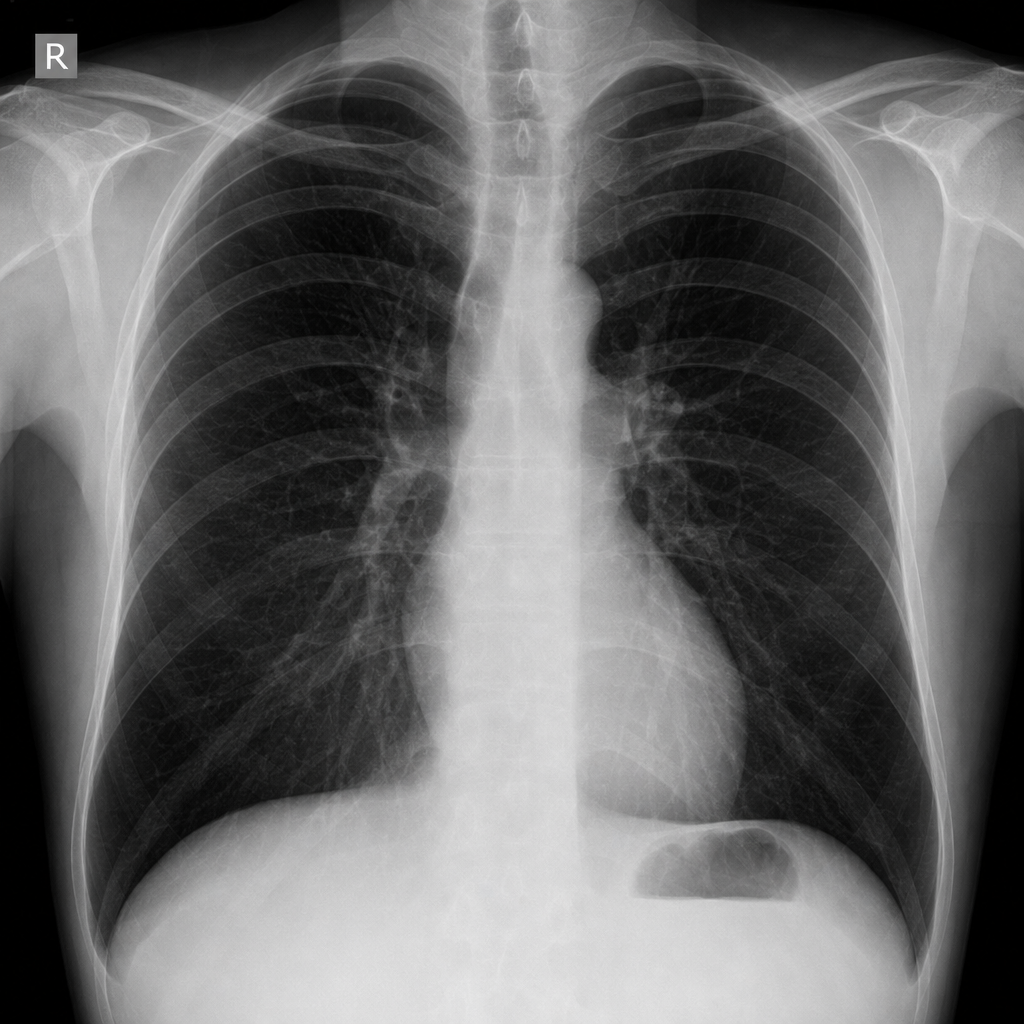
A 55-year-old man with a 60 pack-year smoking history is referred by his primary care physician for a pulmonary function test (PFT). A previously obtained chest x-ray is shown below. Which of the following will most likely appear in his PFT report?
A 50-year-old man presents to the urgent care clinic for 3 hours of worsening cough, shortness of breath, and dyspnea. He works as a long-haul truck driver, and he informs you that he recently returned to the west coast from a trip to Arkansas. His medical history is significant for gout, hypertension, hypercholesterolemia, diabetes mellitus type 2, chronic obstructive pulmonary disease (COPD), and mild intellectual disability. He currently smokes 1 pack of cigarettes/day, drinks a 6-pack of beer/day, and he endorses a past history of injection drug use but currently denies any illicit drug use. The vital signs include: temperature 36.7°C (98.0°F), blood pressure 126/74 mm Hg, heart rate 87/min, and respiratory rate 23/min. His physical examination shows mild, bilateral, coarse rhonchi, but otherwise clear lungs on auscultation, grade 2/6 holosystolic murmur, and a benign abdominal physical examination. He states that he ran out of his albuterol inhaler 6 days ago and has been meaning to follow-up with his primary care physician (PCP) for a refill. Complete blood count (CBC) and complete metabolic panel are within normal limits. He also has a D-dimer result within normal limits. Which of the following is the most appropriate next step in evaluation?
A 63-year-old man presents to the clinic with fever accompanied by shortness of breath. The symptoms developed a week ago and have been progressively worsening over the last 2 days. He reports his cough is productive of thick, yellow sputum. He was diagnosed with chronic obstructive pulmonary disease 3 years ago and has been on treatment ever since. He quit smoking 10 years ago but occasionally experiences shortness of breath along with chest tightness that improves with the use of an inhaler. However, this time the symptoms seem to be more severe and unrelenting. His temperature is 38.6°C (101.4°F), the respirations are 21/min, the blood pressure is 100/60 mm Hg, and the pulse is 105/min. Auscultation reveals bilateral crackles and expiratory wheezes. His oxygen saturation is 95% on room air. According to this patient’s history, which of the following should be the next step in the management of this patient?
A 36-year-old man is seen in the emergency department for back pain that has been getting progressively worse over the last 4 days. Upon further questioning, he also notes that he has been having a tingling and burning sensation rising up from his feet to his knees bilaterally. The patient states he is having difficulty urinating and having bowel movements over the last several days. His temperature is 97.4°F (36.3°C), blood pressure is 122/80 mmHg, pulse is 85/min, respirations are 14/min, and oxygen saturation is 98% on room air. Physical exam is notable for weak leg flexion bilaterally along with decreased anal sphincter tone. Which of the following is the best next step in management?
A 27-year-old man presents to the emergency department with back pain. The patient states that he has back pain that has been steadily worsening over the past month. He states that his pain is worse in the morning but feels better after he finishes at work for the day. He rates his current pain as a 7/10 and says that he feels short of breath. His temperature is 99.5°F (37.5°C), blood pressure is 130/85 mmHg, pulse is 80/min, respirations are 14/min, and oxygen saturation is 99% on room air. On physical exam, you note a young man who does not appear to be in any distress. Cardiac exam is within normal limits. Pulmonary exam is notable only for a minor decrease in air movement bilaterally at the lung bases. Musculoskeletal exam reveals a decrease in mobility of the back in all four directions. Which of the following is the best initial step in management of this patient?
A 65-year-old man is brought to the emergency department with central chest pain for the last hour. He rates his pain as 8/10, dull in character, and says it is associated with profuse sweating and shortness of breath. He used to have heartburn and upper abdominal pain associated with food intake but had never experienced chest pain this severe. He has a history of diabetes, hypertension, and hypercholesterolemia. His current medication list includes amlodipine, aspirin, atorvastatin, insulin, valsartan, and esomeprazole. He has smoked 1 pack of cigarettes per day for the past 35 years. Physical examination reveals: blood pressure 94/68 mm Hg, pulse 112/min, oxygen saturation 95% on room air, and BMI 31.8 kg/m2. His lungs are clear to auscultation. An electrocardiogram (ECG) shows ST-segment elevations in the inferior leads. The patient is discharged home after 3 days on aspirin, clopidogrel, and atenolol in addition to his previous medications. He is advised to get an exercise tolerance test (ETT) in one month. A month later at his ETT, his resting blood pressure is 145/86 mm Hg. The pre-exercise ECG shows normal sinus rhythm with Q waves in the inferior leads. After 3 minutes of exercise, the patient develops chest pain that is gradually worsening, and repeat blood pressure is 121/62 mm Hg. No ischemic changes are noted on the ECG. What is the most appropriate next step?
A 55-year-old man with recurrent pneumonia comes to the physician for a follow-up examination one week after hospitalization for pneumonia. He feels well but still has a productive cough. He has smoked 1 pack of cigarettes daily for 5 years. His temperature is 36.9°C (98.4°F) and respirations are 20/min. Cardiopulmonary examination shows coarse crackles at the right lung base. Microscopic examination of a biopsy specimen of the right lower lung parenchyma shows proliferation of clustered, cuboidal, foamy-appearing cells. These cells are responsible for which of the following functions?
A father brings his 3-year-old son to the pediatrician because he is concerned about his health. He states that throughout his son's life he has had recurrent infections despite proper treatment and hygiene. Upon reviewing the patient's chart, the pediatrician notices that the child has been infected multiple times with S. aureus, Aspergillus, and E. coli. Which of the following would confirm the most likely cause of this patient's symptoms?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app