
Idiopathic pulmonary fibrosis — MCQs

A 57-year-old man comes to the physician because of a 2-month history of worsening shortness of breath with walking. He has not had any cough, fevers, or recent weight loss. He has hypercholesterolemia, for which he takes simvastatin, but otherwise is healthy. For 35 years he has worked for a demolition company. He has smoked 1 pack of cigarettes daily for the past 33 years. Pulmonary examination shows fine bibasilar end-expiratory crackles. An x-ray of the chest shows diffuse bilateral infiltrates predominantly in the lower lobes and bilateral calcified pleural plaques. The patient is most likely to develop which of the following conditions?
A 70-year-old man presents to a physician with a cough and difficulty breathing during the last 7 years. He has smoked since his teenage years and regularly inhales tiotropium, formoterol, and budesonide and takes oral theophylline. The number of exacerbations has been increasing over the last 6 months. His temperature is 37.2°C (99°F), the heart rate is 92/min, the blood pressure is 134/88 mm Hg and the respiratory rate is 26/min. On chest auscultation breath sounds are diffusely decreased and bilateral rhonchi are present. Pulse oximetry shows his resting oxygen saturation to be 88%. Chest radiogram shows a flattened diaphragm, hyperlucency of the lungs, and a long, narrow heart shadow. The physician explains this condition to the patient and emphasizes the importance of smoking cessation. In addition to this, which of the following is most likely to reduce the risk of mortality from the condition?
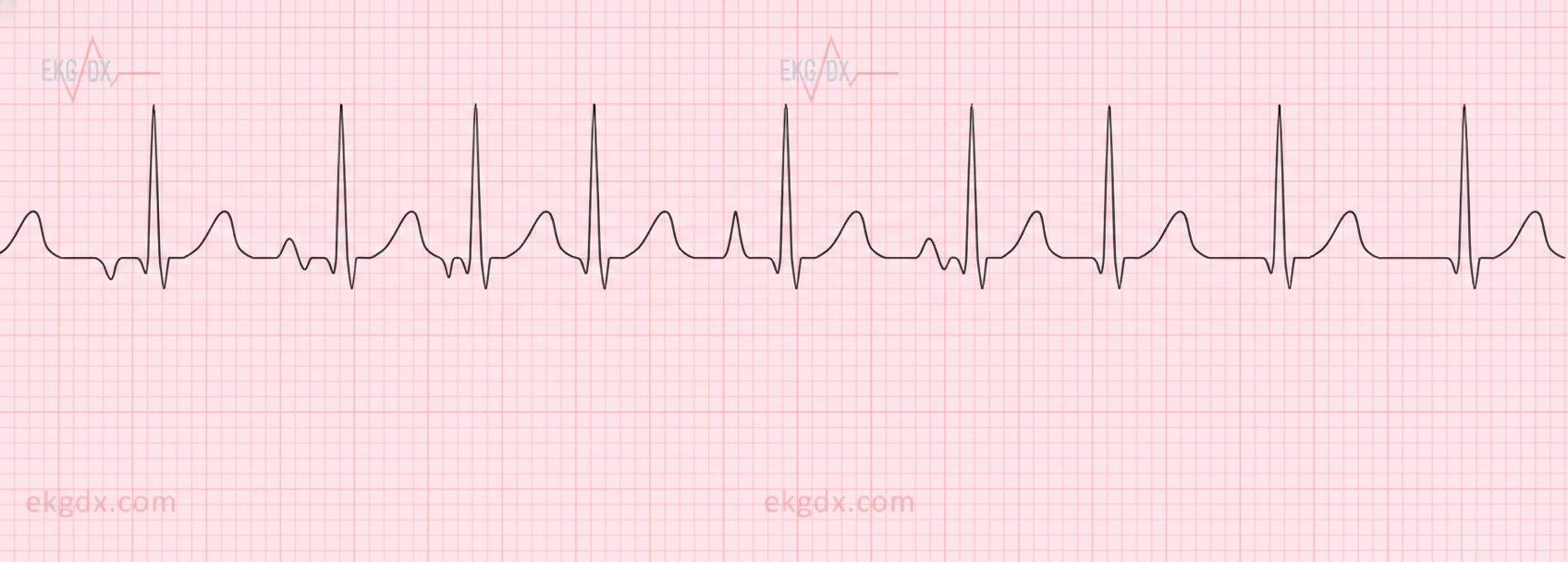
A 62-year-old man with a 5-year history of chronic obstructive pulmonary disease comes to the physician for a follow-up examination. He has had episodic palpitations over the past week. His only medication is a tiotropium-formoterol inhaler. His pulse is 140/min and irregular, respirations are 17/min, and blood pressure is 116/70 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 95%. The lungs are clear to auscultation. Cardiac examination shows no murmurs, rubs, or gallops. Serum concentrations of electrolytes, thyroid-stimulating hormone, and cardiac troponins are within the reference range. An electrocardiogram is shown. Which of the following is the most appropriate next step in management?
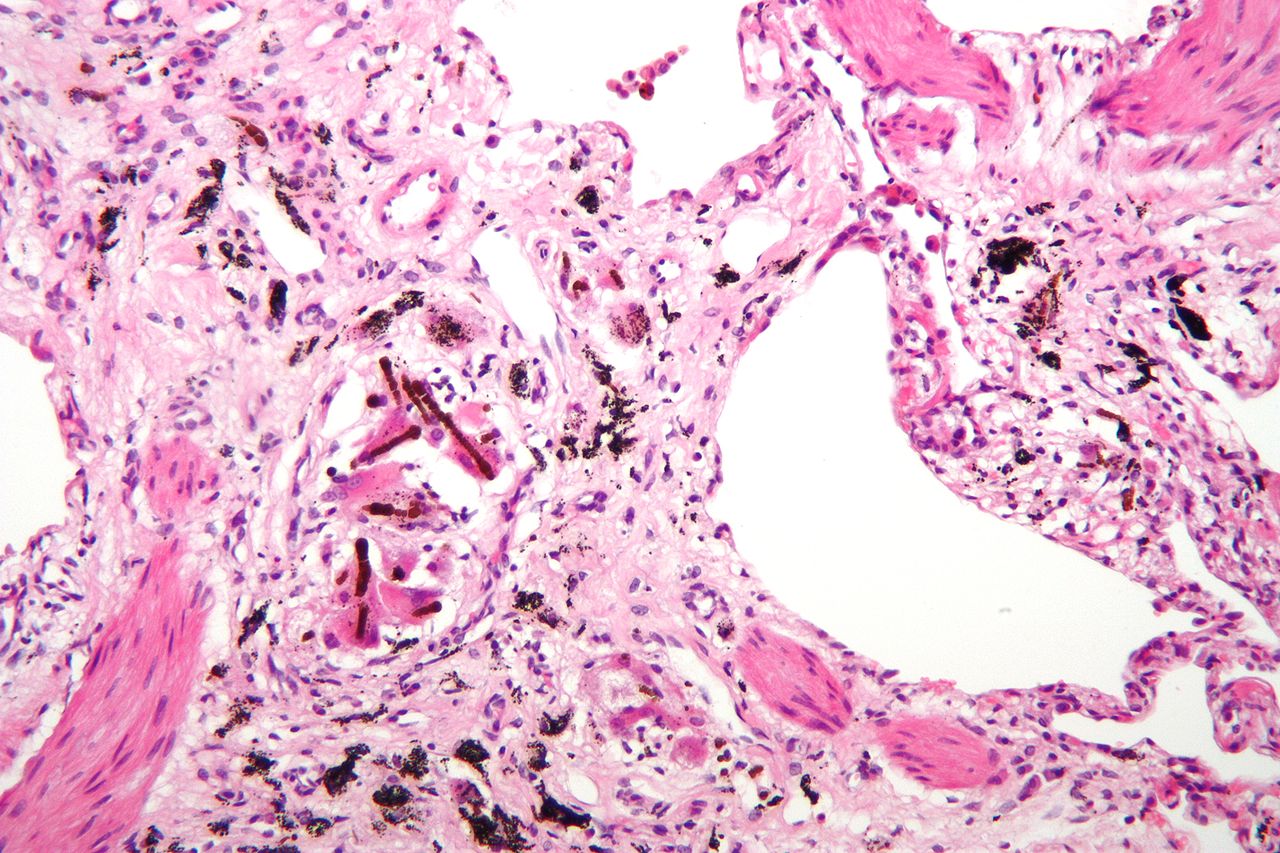
A 61-year-old man comes to the physician because of a 9-month history of progressive shortness of breath on exertion. Pulmonary examinations shows fine bibasilar end-inspiratory crackles. There is digital clubbing. Pulmonary functions tests show an FEV1:FVC ratio of 97% and a total lung capacity of 70%. An x-ray of the chest shows small bilateral reticular opacities, predominantly in the lower lobes. A photomicrograph of a specimen obtained on lung biopsy is shown. The patient most likely works in which of the following fields?
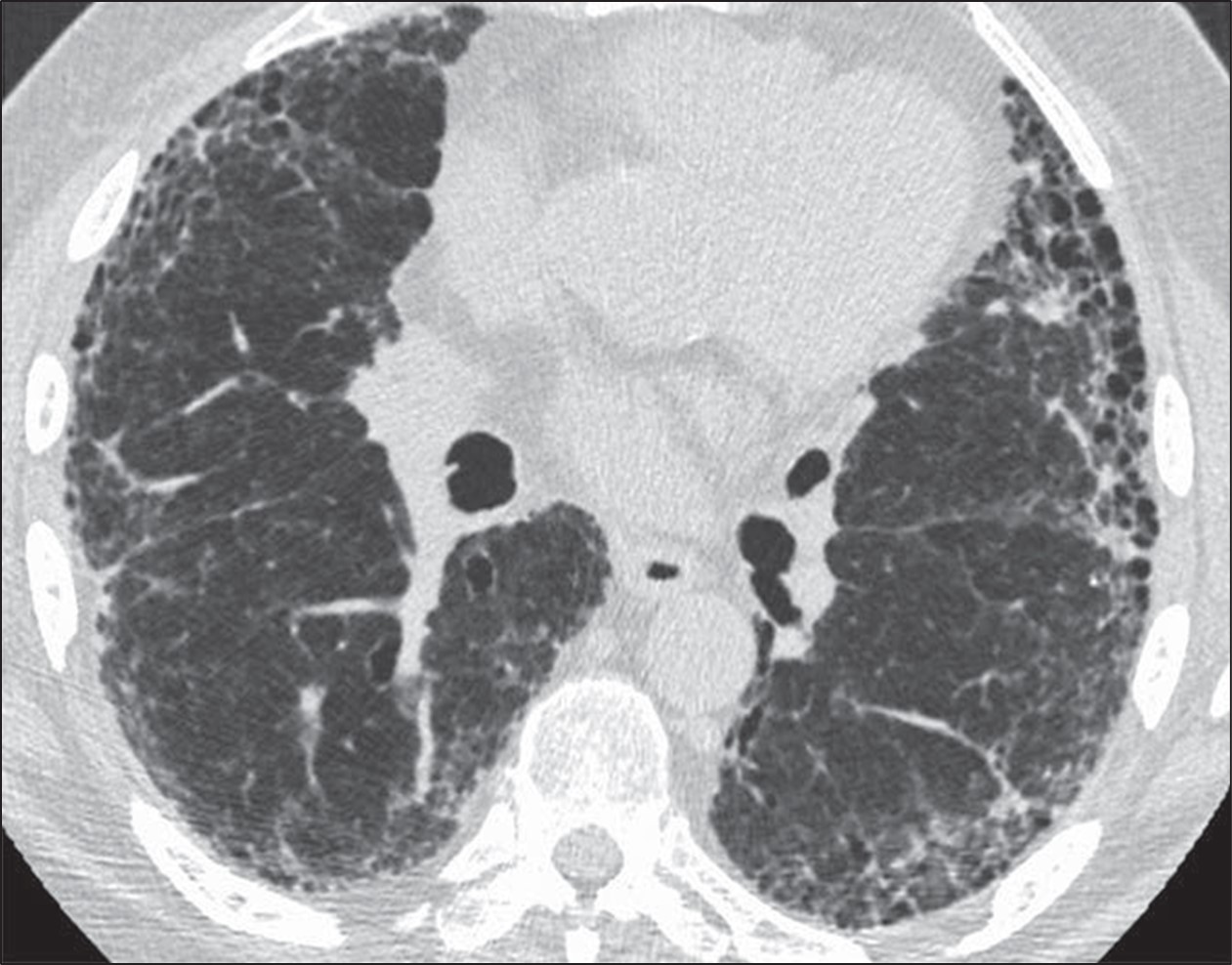
A 52-year-old man comes to the physician because of a 6-month history of shortness of breath and nonproductive cough. He has smoked 1 pack of cigarettes daily for 15 years. Cardiopulmonary examination shows fine inspiratory crackles bilaterally. There is clubbing present in the fingers bilaterally. Pulmonary function tests (PFTs) show an FVC of 78% of expected and an FEV1/FVC ratio of 92%. A CT scan of the chest is shown. Which of the following is the most likely underlying diagnosis?
A 33-year-old African-American female presents to her physician with complaints of a persistent, dry cough. She states that the cough has gone on for some time now. Three weeks ago, during her last general checkup, she was started on lisinopril and metformin for concerns regarding an elevated blood pressure and fasting blood glucose. Past medical history is notable for eczema, asthma, and seasonal allergies. At this visit the patient has other non-specific complaints such as fatigue and joint pain as well as a burning sensation in her sternum when she eats large meals. Her physical exam is only notable for painful bumps on her lower extremities (figure A) which the patient attributes to "bumping her shins," during exercise, and an obese habitus. Which of the following is most likely true for this patient's chief concern?

A 65-year-old male engineer presents to the office with shortness of breath on exertion and a dry cough that he has had for about a year. He is a heavy smoker with a 25-pack-years history. His vitals include: heart rate 95/min, respiratory rate 26/min, and blood pressure 110/75 mm Hg. On examination, he presents with nail clubbing and bilateral and persistent crackling rales. The chest radiograph shows basal reticulonodular symmetric images, with decreased lung fields. The pulmonary function tests show the following: diffusing capacity of the lungs for carbon monoxide (DLCO) is 43% and reference SaO2 is 94% and 72%, at rest and with exercise, respectively. What is the most likely diagnosis?
A 61-year-old male presents to your office with fever and dyspnea on exertion. He has been suffering from chronic, non-productive cough for 1 year. You note late inspiratory crackles on auscultation. Pulmonary function tests reveal an FEV1/FVC ratio of 90% and an FVC that is 50% of the predicted value. Which of the following would you most likely see on a biopsy of this patient's lung?
A 52-year-old man is brought to the emergency department by a friend because of a 5-day history of fever and cough productive of purulent sputum. One week ago, he was woken up by an episode of heavy coughing while lying on his back. He drinks large amounts of alcohol daily and has spent most of his time in bed since his wife passed away 2 months ago. His temperature is 38°C (100.4°F), pulse is 96/min, respirations are 24/min, and blood pressure is 110/84 mm Hg. Pulse oximetry on room air shows an oxygen saturation of 87%. Physical examination shows poor dentition and swollen gums. A CT scan of the chest is most likely to show a pulmonary infiltrate in which of the following locations?
A 27-year-old woman with a history of a "heart murmur since childhood" presents following a series of syncopal episodes over the past several months. She also complains of worsening fatigue over this time period, and notes that her lips have begun to take on a bluish tinge, for which she has been using a brighter shade of lipstick. You do a careful examination, and detect a right ventricular heave, clubbing of the fingers, and 2+ pitting edema bilaterally to the shins. Despite your patient insisting that every doctor she has ever seen has commented on her murmur, you do not hear one. Transthoracic echocardiography would most likely detect which of the following?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app