
COPD management and exacerbations — MCQs

A 63-year-old man presents to the clinic with fever accompanied by shortness of breath. The symptoms developed a week ago and have been progressively worsening over the last 2 days. He reports his cough is productive of thick, yellow sputum. He was diagnosed with chronic obstructive pulmonary disease 3 years ago and has been on treatment ever since. He quit smoking 10 years ago but occasionally experiences shortness of breath along with chest tightness that improves with the use of an inhaler. However, this time the symptoms seem to be more severe and unrelenting. His temperature is 38.6°C (101.4°F), the respirations are 21/min, the blood pressure is 100/60 mm Hg, and the pulse is 105/min. Auscultation reveals bilateral crackles and expiratory wheezes. His oxygen saturation is 95% on room air. According to this patient’s history, which of the following should be the next step in the management of this patient?
A 48-year-old man presents with a productive cough and occasional dyspnea on exertion. He has experienced these symptoms for the past 6 years. Patient denies weight loss, night sweats, or hemoptysis. Past medical history is significant for arterial hypertension, diagnosed 3 years ago, and diabetes mellitus type 2, diagnosed 5 years ago. He also has allergic rhinitis with exacerbations in the spring. The current medications include 12.5 mg of lisinopril and 1,000 mg of metformin daily. The patient reports a 30-pack-year smoking history. He works as a financial advisor and is physically inactive. The vital signs are within normal limits. The BMI is 44.9 kg/m2. Upon physical examination, lung auscultation is significant for occasional wheezes over both lungs. The spirometry shows an FEV1 of 59% of predicted. Which of the following interventions would be most useful to slow the progression of this patient’s most likely condition?
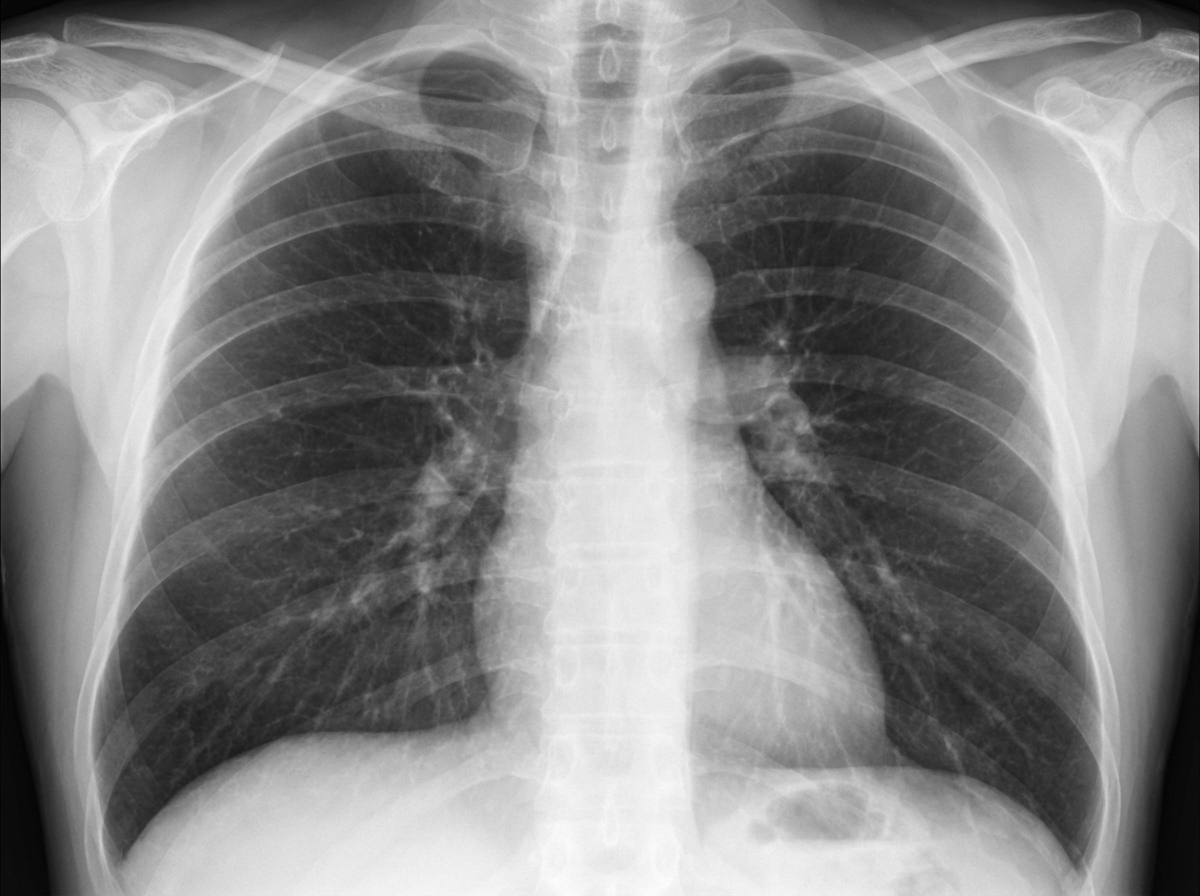
A 28-year-old patient presents to the hospital complaining of progressively worsening dyspnea and a dry cough. Radiographic imaging is shown below. Pulmonary function testing (PFT's) reveals a decreased FEV1 and FEV1/FVC, but an increased TLC. The patient states that he does not smoke. Which of the following conditions is most consistent with the patient's symptoms?
A 36-year-old woman comes to the physician because of a 3-month history of intermittent cough productive of thick, yellow phlegm and increasing shortness of breath. She especially becomes short of breath while playing with her children. She has worked as a farmer for 18 years. She has asthma treated with a salbutamol inhaler. She has smoked half a pack of cigarettes daily for 12 years. Her pulse is 65/min, respirations are 14/min, and blood pressure is 110/75 mm Hg. Scattered wheezing and decreased breath sounds are heard throughout both lung fields. Cardiac examination shows no abnormalities. The abdomen is soft and nondistended; liver span in midclavicular line is 14 cm.Spirometry shows a FEV1:FVC ratio of 66% and a FEV1 of 50% of predicted. An x-ray of the chest is shown. Which of the following is the most likely underlying cause of this patient's condition?
A 57-year-old woman presents to her physician’s office because she is coughing up blood. She says that she first observed a somewhat reddish sputum a few months ago. However, over the past couple of weeks, the amount of blood she coughs has significantly increased. She has been smoking for the past 30 years. She says that she smokes about 2 packs of cigarettes daily. She does not have fever, night sweats, weight loss, or chills. She reports progressive difficulty in breathing. On examination, her vital signs are stable. On auscultation of her chest, she has an expiratory wheeze. Oxygen saturation is 98%. Which of the following would be the next best step in the management of this patient?
A 21-year-old woman comes to the physician for the evaluation of dry cough and some chest tightness for the past several weeks. The cough is worse at night and while playing volleyball. She frequently has a runny nose and nasal congestion. Her mother has systemic lupus erythematosus. The patient has smoked one pack of cigarettes daily for the last 5 years. She does not drink alcohol. Her only medication is cetirizine. Her vital signs are within normal limits. Pulse oximetry on room air shows an oxygen saturation of 98%. The remainder of the examination shows no abnormalities. Which of the following is the most appropriate next step in management?
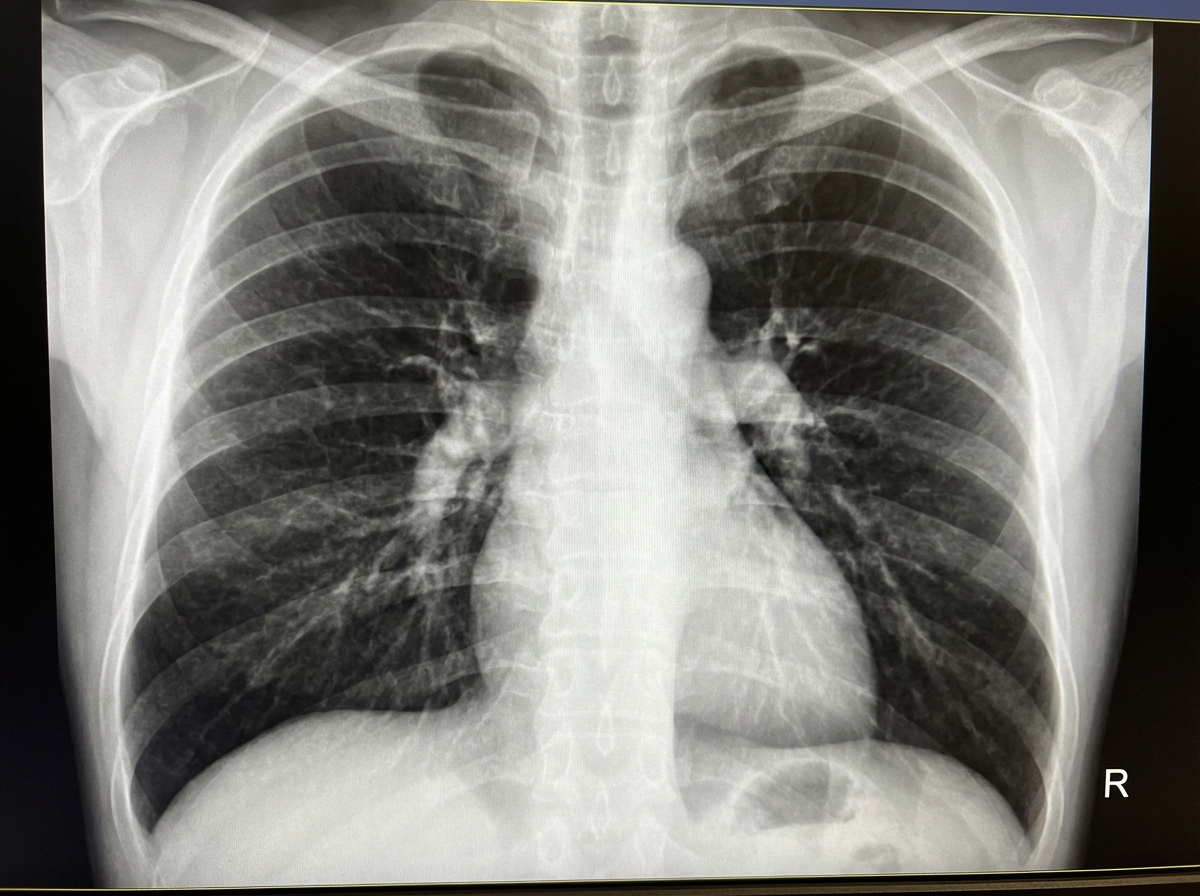
A 68-year-old man presents with shortness of breath, particularly when walking up stairs and when lying down to go to sleep at night. He also complains of a chronic cough and states that he now uses 2 extra pillows at night. The patient has a history of type 2 diabetes that is well-managed with metformin. He also takes Prozac for a long-standing history of depression. The patient has a 60-pack-year smoking history. He also has a history significant for alcohol abuse, but he quit cold turkey 15 years ago when his brother was killed in a drunk driving accident. Both he and his brother were adopted, and he does not know other members of his biological family. Despite repeated efforts of patient counseling, the patient is not interested in quitting smoking. The physical exam is significant for an obese male using accessory muscles of respiration. The vital signs include: temperature 36.8°C (98.2°F), heart rate 95/min, respiratory rate 16/min, and blood pressure 130/85 mm Hg. The oxygen saturation is 90% on room air. Additional physical exam findings include cyanotic lips, peripheral edema, hepatomegaly, and ascites. The cardiovascular exam is significant for an S3 heart sound and elevated JVP. The pulmonary exam is significant for expiratory wheezing, diffuse rhonchi, and hyperresonance on percussion. The laboratory test results are as follows: BUN 15 mg/dL pCO2 60 mm Hg Bicarbonate (HCO3) 32 mmol/L Creatinine 0.8 mg/dL Glucose 95 mg/dL Serum chloride 103 mmol/L Serum potassium 3.9 mEq/L Serum sodium 140 mEq/L Total calcium 2.3 mmol/L Hemoglobin 26 g/dL Bilirubin total 0.9 mg/dL Bilirubin indirect 0.4 mg/dL Iron 100 Ferritin 70 TIBC 300 The posterior-anterior chest X-ray is shown in the image. Which of the following interventions is indicated for decreasing the mortality of this patient?
A 32-year-old man is brought into the emergency department by his friends. The patient was playing soccer when he suddenly became short of breath. The patient used his albuterol inhaler with minimal improvement in his symptoms. He is currently struggling to breathe. The patient has a past medical history of asthma and a 25 pack-year smoking history. His current medications include albuterol, fluticasone, and oral prednisone. His temperature is 99.5°F (37.5°C), blood pressure is 137/78 mmHg, pulse is 120/min, respirations are 27/min, and oxygen saturation is 88% on room air. On pulmonary exam, the patient exhibits no wheezing with bilateral minimal air movement. The patient’s laboratory values are ordered as seen below. Hemoglobin: 15 g/dL Hematocrit: 43% Leukocyte count: 5,500/mm^3 with normal differential Platelet count: 194,000/mm^3 Serum: Na+: 138 mEq/L Cl-: 102 mEq/L K+: 4.4 mEq/L HCO3-: 24 mEq/L BUN: 20 mg/dL Glucose: 120 mg/dL Creatinine: 1.0 mg/dL Ca2+: 10.2 mg/dL pH: 7.44 PaCO2: 10 mmHg PaO2: 60 mmHg AST: 12 U/L ALT: 10 U/L The patient is started on an albuterol nebulizer, magnesium sulfate, and tiotropium bromide. Repeat vitals reveal an oxygen saturation of 90% with a pulse of 115/min. Laboratory values are repeated as seen below. pH: 7.40 PaCO2: 44 mmHg PaO2: 64 mmHg Which of the following is the next best step in management of this patient?
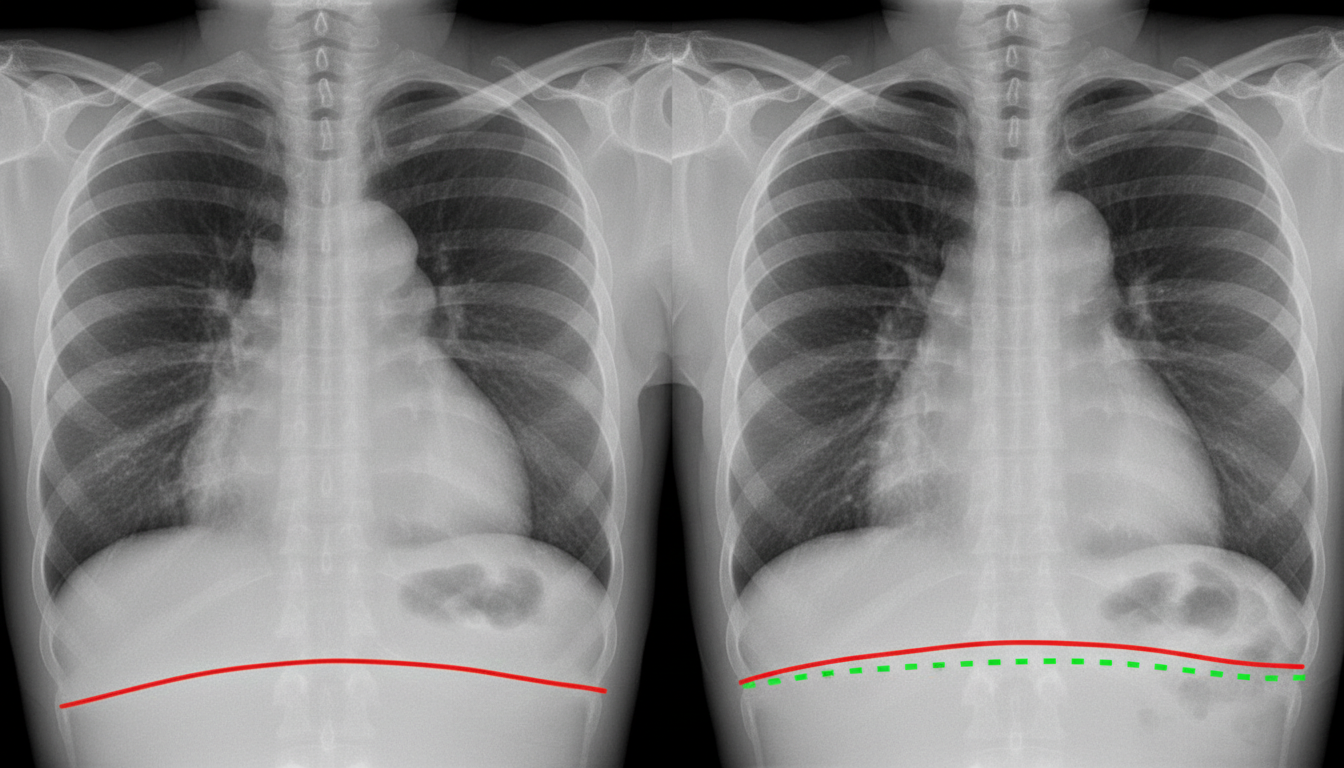
A 40-year-old man comes to the physician because of a 2-year history of gradually worsening shortness of breath. He smoked half a pack of cigarettes daily for 10 years but stopped 8 years ago. His pulse is 72/min, blood pressure is 135/75 mm Hg, and respirations are 20/min. Examination shows an increased anteroposterior diameter of the chest. Diminished breath sounds are heard on auscultation of the chest. An x-ray of the chest shows widened intercostal spaces, a flattened diaphragm, and bilateral hyperlucency of the lung bases. This patient's condition puts him at greatest risk for which of the following conditions?
A 65-year-old man comes to the physician for a follow-up examination. He has chronic obstructive pulmonary disease and was recently discharged from the hospital for an exacerbation. His cough and chills have since improved, but his mobility is still severely limited by dyspnea and fatigue. He smoked 2 packs of cigarettes daily for 30 years, but quit 5 years ago. His medications include inhaled daily budesonide, formoterol, and tiotropium bromide plus ipratropium/albuterol as needed. Pulmonary function testing shows an FEV1 of 27% of predicted. Resting oxygen saturation ranges from 84–88%. Which of the following steps in management is most likely to increase the chance of survival in this patient?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app