
Pancreatitis — MCQs

On this page
A 70-year-old male visits his primary care physician because of progressive weight loss. He has a 20-year history of smoking 2 packs of cigarettes a day and was diagnosed with diabetes mellitus 6 years ago. After physical examination, the physician tells the patient he suspects adenocarcinoma at the head of the pancreas. Which of the following physical examination findings would support the diagnosis?
A 45-year-old man with a history of biliary colic presents with one-day of intractable nausea, vomiting, and abdominal pain radiating to the back. Temperature is 99.7 deg F (37.6 deg C), blood pressure is 102/78 mmHg, pulse is 112/min, and respirations are 22/min. On abdominal exam, he has involuntary guarding and tenderness to palpation in the right upper quadrant and epigastric regions. Laboratory studies show white blood cell count 18,200/uL, alkaline phosphatase 650 U/L, total bilirubin 2.5 mg/dL, amylase 500 U/L, and lipase 1160 U/L. Which of the patient's laboratory findings is associated with increased mortality?
A 36-year-old man is brought to the emergency department 3 hours after the onset of progressively worsening upper abdominal pain and 4 episodes of vomiting. His father had a myocardial infarction at the age of 40 years. Physical examination shows tenderness and guarding in the epigastrium. Bowel sounds are decreased. His serum amylase is 400 U/L. Symptomatic treatment and therapy with fenofibrate are initiated. Further evaluation of this patient is most likely to show which of the following findings?
A 29-year-old female is hospitalized 1 day after an endoscopic retrograde cholangiopancreatography (ERCP) because of vomiting, weakness, and severe abdominal pain. Physical examination findings include abdominal tenderness and diminished bowel sounds. A CT scan demonstrates fluid around the pancreas. Serum levels of which of the following are likely to be low in this patient?
A 65-year-old woman comes to the physician because of a 1-month history of persistent epigastric abdominal pain. She reports dull, aching pain that is worse after meals and wakes her up at night. She is afraid to eat, as it worsens the pain, and has had a 2-kg (4.4-lb) weight loss during this time. She has smoked a pack of cigarettes daily for the past 40 years. Her only medication is a calcium supplement. Her vital signs are within normal limits. She appears thin. Examination shows yellow discoloration of the sclera. The remainder of the examination shows no abnormalities. Laboratory studies show a total bilirubin of 9.8 mg/dL, direct bilirubin of 8.6 mg/dL, and an alkaline phosphatase of 120 IU/L. Abdominal ultrasonography shows dilation of the biliary and pancreatic ducts but no pancreatic or extrahepatic biliary lesions. Which of the following is the most appropriate next step in management?
A 54-year-old woman presents to the emergency room after falling on her right side at a bar and breaking her clavicle and 2 ribs. Her husband reports that she has had a 6-month history of diarrhea and has lost 6.8 kg (15 lb) over the last year without dieting or exercising. She has a family history of type I diabetes. On physical exam, ecchymosis is noted over her entire right shoulder, extending to her sternum and over her broken ribs. She also has other bruises in various stages of healing. Her abdomen is diffusely tender, radiating to her back, and there is a palpable midepigastric mass. The woman has a positive Romberg test, but the rest of her examination is normal. She is admitted for further evaluation. Her labs and pancreas biopsy histology are as follows: Laboratory tests Serum chemistries Albumin 5.1 g/dL Amylase 124 U/L Lipase 146 U/L Blood glucose (fasting) 180 mg/dL Triglycerides 140 mg/dL Cholesterol, total 210 mg/dL HDL 25 mg/dL LDL 165 mg/dL Serum electrolytes Sodium 137 mEq/L Potassium 3.5 mEq/L Chloride 90 mEq/L International normalized ratio 2.5 Activated partial thromboplastin time 30 s Complete blood count Hemoglobin 12.5 g/dL Mean corpuscular volume 102 µm3 Platelets 150,000/mm3 Leukocytes 6000/mm3 Stool analysis Elastase low Occult blood absent Which of the following is the best way to manage her condition in the long term?
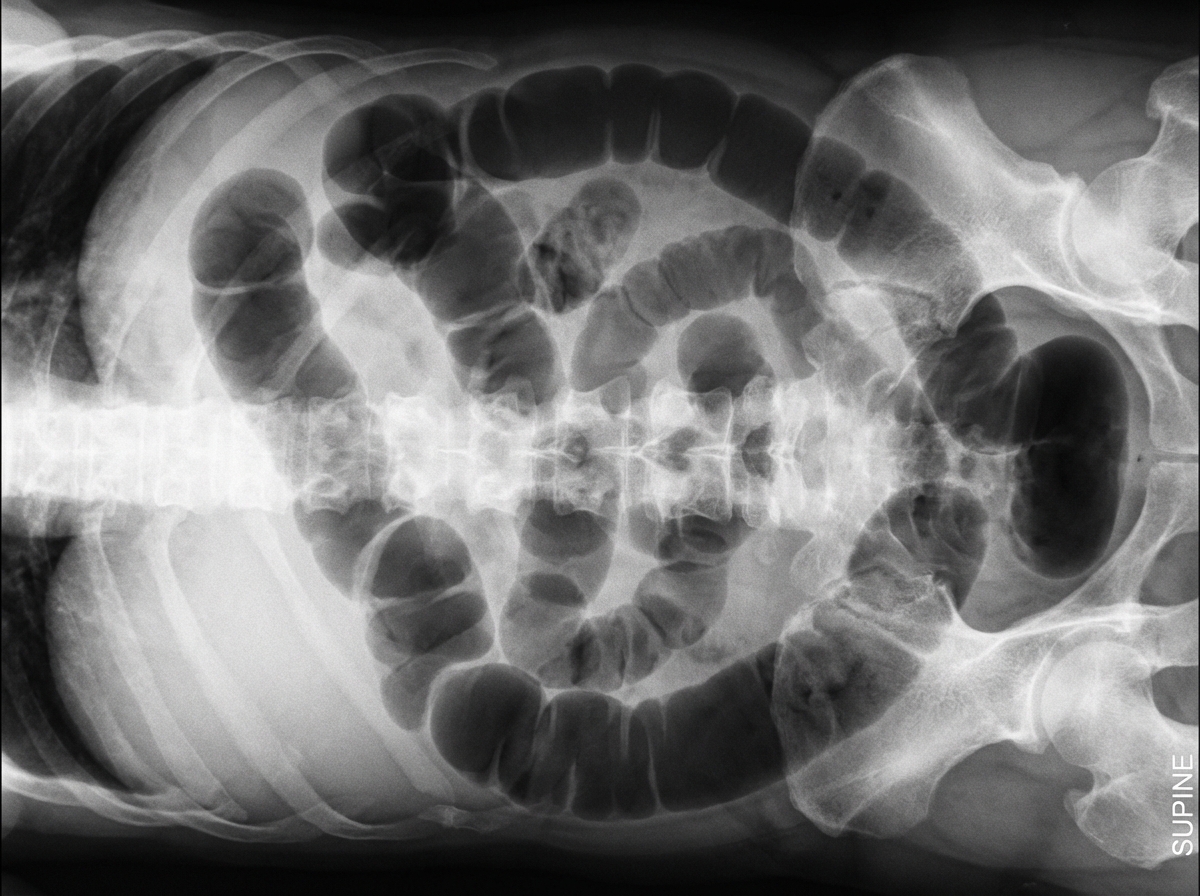
A 45-year-old woman has painless abdominal distension 2 days after admission for acute pancreatitis. Her initial abdominal pain has resolved. Enteral nutrition has been initiated. She has not passed any stool since being admitted to the hospital. She has nausea but no vomiting. Her temperature is 36.7°C (98.1°F), pulse is 95/min, respiratory rate is 17/min, and blood pressure is 100/70 mm Hg. The lungs are clear to auscultation. Abdominal examination shows symmetric distention, absent bowel sounds, and tympanic percussion without tenderness. Laboratory studies show: Serum Na+ 137 mEq/L K+ 3.2 mEq/L Cl− 104 mEq/L HCO3− 23 mEq/L Urea nitrogen 22 mg/dL Creatinine 0.8 mg/dL A supine abdominal X-ray is shown. Which of the following best explains these findings?
A 72-year-old woman comes to the emergency department because of upper abdominal pain and nausea for the past hour. The patient rates the pain as an 8 to 9 on a 10-point scale. She has had an episode of nonbloody vomiting since the pain started. She has a history of type 2 diabetes mellitus, hypertension, and osteoporosis. The patient has smoked 2 packs of cigarettes daily for 40 years. She drinks 5–6 alcoholic beverages daily. Current medications include glyburide, lisinopril, and oral vitamin D supplements. Her temperature is 38.5°C (101.3°F), pulse is 110/min, and blood pressure is 138/86 mm Hg. Examination shows severe epigastric tenderness to palpation with guarding but no rebound. Ultrasonography of the abdomen shows diffuse enlargement of the pancreas; no gallstones are visualized. The patient is admitted to the hospital for pain control and intravenous hydration. Which of the following is the most appropriate next step in the management of this patient’s pain?
A 49-year-old woman comes to the physician because of difficulty walking and dizziness for the past 2 weeks. She has also had fatigue, heartburn, and diarrhea for 4 months. The stools are foul-smelling and do not flush easily. Over the past 4 months, she has had a 2.2-kg (5-lb) weight loss. Her only medication is an over-the-counter antacid. Her mother has autoimmune thyroid disease and Crohn disease. She is 150 cm (4 ft 11 in) tall and weighs 43 kg (95 lb); BMI is 19.1 kg/m2. Vital signs are within normal limits. Examination shows a wide-based gait. Muscle strength and tone are normal in all extremities. Rapid alternating movement of the hands is impaired. The abdomen is soft and there is mild tenderness to palpation in the epigastric area. Her hemoglobin concentration is 11.1 mg/dL, and levels of vitamin E and vitamin D are decreased. Upper endoscopy shows several ulcers in the gastric antrum and the descending duodenum. Which of the following is the most likely underlying mechanism of this patient's symptoms?
A 72-year-old man is brought to the physician by his son because of gradually progressive yellow discoloration of his skin and generalized pruritus for the past 2 weeks. During this period, his appetite has decreased and he has had a 6.3-kg (14-lb) weight loss. He reports that his stool appears pale and his urine is very dark. Three years ago, he had an episode of acute upper abdominal pain that was treated with IV fluids, NSAIDs, and dietary modification. He has stopped drinking alcohol since then; he used to drink 1–2 beers daily for 40 years. He has smoked a pack of cigarettes daily for the past 50 years. His vital signs are within normal limits. Physical examination shows yellowing of the conjunctivae and skin. The abdomen is soft and nontender; a soft, cystic mass is palpated in the right upper quadrant. Serum studies show: Bilirubin, total 5.6 mg/dL Direct 4.8 mg/dL Alkaline phosphatase 192 U/L AST 32 U/L ALT 34 U/L Abdominal ultrasonography shows an anechoic cystic mass in the subhepatic region and dilation of the intrahepatic and extrahepatic bile ducts. Which of the following is the most likely diagnosis?
Practice by Chapter
Acute pancreatitis etiology
Practice Questions
Acute pancreatitis diagnosis
Practice Questions
Severity assessment in acute pancreatitis
Practice Questions
Management of acute pancreatitis
Practice Questions
Local complications of acute pancreatitis
Practice Questions
Systemic complications of acute pancreatitis
Practice Questions
Chronic pancreatitis pathophysiology
Practice Questions
Diagnosis of chronic pancreatitis
Practice Questions
Pain management in chronic pancreatitis
Practice Questions
Exocrine pancreatic insufficiency
Practice Questions
Endocrine complications in pancreatitis
Practice Questions
Autoimmune pancreatitis
Practice Questions
Pancreatic cancer risk in chronic pancreatitis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app