
Exocrine pancreatic insufficiency — MCQs

A 29-year-old female is hospitalized 1 day after an endoscopic retrograde cholangiopancreatography (ERCP) because of vomiting, weakness, and severe abdominal pain. Physical examination findings include abdominal tenderness and diminished bowel sounds. A CT scan demonstrates fluid around the pancreas. Serum levels of which of the following are likely to be low in this patient?
An 82-year-old woman presents with 2 months of foul-smelling, greasy diarrhea. She says that she also has felt very tired recently and has had some associated bloating and flatus. She denies any recent abdominal pain, nausea, melena, hematochezia, or vomiting. She also denies any history of recent travel and states that her home has city water. Which of the following tests would be most appropriate to initially work up the most likely diagnosis in this patient?
A 55-year-old woman presents with acute onset abdominal pain radiating to her back, nausea, and vomiting. CT scan suggests a diagnosis of acute pancreatitis. The pathogenesis of acute pancreatitis relates to inappropriate activation of trypsinogen to trypsin. Which of the following activates trypsin in normal digestion?
A 49-year-old woman comes to the physician because of difficulty walking and dizziness for the past 2 weeks. She has also had fatigue, heartburn, and diarrhea for 4 months. The stools are foul-smelling and do not flush easily. Over the past 4 months, she has had a 2.2-kg (5-lb) weight loss. Her only medication is an over-the-counter antacid. Her mother has autoimmune thyroid disease and Crohn disease. She is 150 cm (4 ft 11 in) tall and weighs 43 kg (95 lb); BMI is 19.1 kg/m2. Vital signs are within normal limits. Examination shows a wide-based gait. Muscle strength and tone are normal in all extremities. Rapid alternating movement of the hands is impaired. The abdomen is soft and there is mild tenderness to palpation in the epigastric area. Her hemoglobin concentration is 11.1 mg/dL, and levels of vitamin E and vitamin D are decreased. Upper endoscopy shows several ulcers in the gastric antrum and the descending duodenum. Which of the following is the most likely underlying mechanism of this patient's symptoms?
A 46-year-old man is brought to the emergency department because of severe epigastric pain and vomiting for the past 4 hours. The pain is constant, radiates to his back, and is worse on lying down. He has had 3–4 episodes of greenish-colored vomit. He was treated for H. pylori infection around 2 months ago with triple-regimen therapy. He has atrial fibrillation and hypertension. He owns a distillery on the outskirts of a town. The patient drinks 4–5 alcoholic beverages daily. Current medications include dabigatran and metoprolol. He appears uncomfortable. His temperature is 37.8°C (100°F), pulse is 102/min, and blood pressure is 138/86 mm Hg. Examination shows severe epigastric tenderness to palpation with guarding but no rebound. Bowel sounds are hypoactive. Rectal examination shows no abnormalities. Laboratory studies show: Hematocrit 53% Leukocyte count 11,300/mm3 Serum Na+ 133 mEq/L Cl- 98 mEq/L K+ 3.1 mEq/L Calcium 7.8 mg/dL Urea nitrogen 43 mg/dL Glucose 271 mg/dL Creatinine 2.0 mg/dL Total bilirubin 0.7 mg/dL Alkaline phosphatase 61 U/L AST 19 U/L ALT 17 U/L γ-glutamyl transferase (GGT) 88 u/L (N=5–50 U/L) Lipase 900 U/L (N=14–280 U/L) Which of the following is the most appropriate next step in management?
A 34-year-old woman comes to the emergency department because of decreased appetite, nausea, vomiting, and episodic abdominal pain for the past two months. The pain is sharp, colicky, and lasts about an hour after meals. Her stools are light in appearance and difficult to flush. Physical examination shows tenderness in the right upper quadrant. Without treatment, this patient is at greatest risk for developing which of the following?
A 62-year-old Caucasian man visits his primary care provider with recurrent episodes of moderate to severe abdominal pain, nausea, and anorexia for the past 2 years. Additional complaints include constipation, steatorrhea, weight loss, polyphagia, and polyuria. His personal history is relevant for a 2-year period of homelessness when the patient was 55 years old, cigarette smoking since the age of 20, alcohol abuse, and cocaine abuse for which is currently under the supervision of a psychiatry team. He has a pulse of 70/min, a respiratory rate of 16/min, a blood pressure of 130/70 mm Hg, and a body temperature of 36.4°C (97.5°F). His height is 178 cm (5 ft 10 in) and weight is 90 kg (198 lb). On physical examination, he is found to have telangiectasias over the anterior chest, mild epigastric tenderness, and a small nodular liver. Laboratory test results from his previous visit a month ago are shown below: Fasting plasma glucose 160 mg/dL HbA1c 8% Serum triglycerides 145 mg/dL Total cholesterol 250 mg/dL Total bilirubin 0.8 mg/dL Direct bilirubin 0.2 mg/dL Amylase 180 IU/L Lipase 50 IU/L Stool negative for blood; low elastase This patient’s condition is most likely secondary to which of the following conditions?
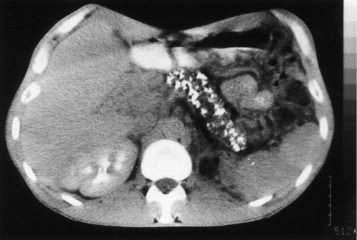
A 42-year-old man comes to the physician because of severe epigastric pain for a week. The pain is constant and he describes it as 6 out of 10 in intensity. The pain radiates to his back and is worse after meals. He has had several episodes of nausea and vomiting during this period. He has taken ibuprofen for multiple similar episodes of pain during the past 6 months. He also has had a 5.4-kg (12-lb) weight loss over the past 4 months. He has a 12-year history of drinking 3 to 4 pints of rum daily. He has been hospitalized three times for severe abdominal pain in the past 3 years. He appears ill. His temperature is 37°C (98.6°F), pulse is 87/min, and blood pressure is 110/70 mm Hg. There is severe epigastric tenderness to palpation. Bowel sounds are normal. Cardiopulmonary examination shows no abnormalities. Laboratory studies show: Hemoglobin 13.6 g/dL Leukocyte count 7,800/mm3 Serum Glucose 106 mg/dL Creatinine 1.1 mg/dL Amylase 150 U/L A CT of the abdomen is shown. Which of the following is the most appropriate long-term management for this patient?
A 42-year-old female with a history of systemic lupus erythematosus (SLE) has a 3-year history of daily prednisone (20 mg) use. Due to long-term prednisone use, she is at increased risk for which of the following?
A 2720-g (6-lb) female newborn delivered at 35 weeks’ gestation starts vomiting and becomes inconsolable 48 hours after birth. The newborn has not passed her first stool yet. Examination shows abdominal distention and high-pitched bowel sounds. A water-soluble contrast enema study shows microcolon. Serum studies show increased levels of immunoreactive trypsinogen. Which of the following is the most likely additional laboratory finding?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app