
Chronic pancreatitis pathophysiology — MCQs

A 29-year-old female is hospitalized 1 day after an endoscopic retrograde cholangiopancreatography (ERCP) because of vomiting, weakness, and severe abdominal pain. Physical examination findings include abdominal tenderness and diminished bowel sounds. A CT scan demonstrates fluid around the pancreas. Serum levels of which of the following are likely to be low in this patient?
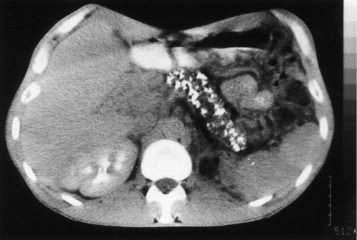
A 42-year-old man comes to the physician because of severe epigastric pain for a week. The pain is constant and he describes it as 6 out of 10 in intensity. The pain radiates to his back and is worse after meals. He has had several episodes of nausea and vomiting during this period. He has taken ibuprofen for multiple similar episodes of pain during the past 6 months. He also has had a 5.4-kg (12-lb) weight loss over the past 4 months. He has a 12-year history of drinking 3 to 4 pints of rum daily. He has been hospitalized three times for severe abdominal pain in the past 3 years. He appears ill. His temperature is 37°C (98.6°F), pulse is 87/min, and blood pressure is 110/70 mm Hg. There is severe epigastric tenderness to palpation. Bowel sounds are normal. Cardiopulmonary examination shows no abnormalities. Laboratory studies show: Hemoglobin 13.6 g/dL Leukocyte count 7,800/mm3 Serum Glucose 106 mg/dL Creatinine 1.1 mg/dL Amylase 150 U/L A CT of the abdomen is shown. Which of the following is the most appropriate long-term management for this patient?
A 29-year-old woman presents with a 2-hour history of sudden onset of severe mid-epigastric pain. The pain radiates to the back, and is not relieved by over-the-counter antacids. The patient also complains of profuse vomiting. The patient’s medical history is negative for similar symptoms. She consumes 3–4 alcoholic drinks daily. The blood pressure is 80/40 mm Hg and the heart rate is 105/min. Examination of the lungs reveals bibasilar crackles. Abdominal examination reveals diffuse tenderness involving the entire abdomen, marked guarding, rigidity, and reduced bowel sounds. The chest X-ray is normal. However, the abdominal CT scan reveals peritoneal fluid collection and diffuse pancreatic enlargement. The laboratory findings include: Aspartate aminotransferase 63 IU/L Alkaline phosphatase 204 IU/L Alanine aminotransferase 32 IU/L Serum amylase 500 IU/L (Normal: 25-125 IU/L) Serum lipase 1,140 IU/L (Normal: 0-160 IU/L) Serum calcium 2 mmol/L Which of the following cellular changes are most likely, based on the clinical and laboratory findings?
A 28-year-old man presents to the emergency department with diffuse abdominal pain and nausea for the past 5 hours. The pain started with a dull ache but is now quite severe. He notes that he “just doesn’t feel like eating” and has not eaten anything for almost a day. Although the nausea is getting worse, the patient has not vomited. He notes no medical issues in the past and is not currently taking any medications. He admits to drinking alcohol (at least 2–3 bottles of beer per day after work and frequent binge-drinking weekends with friends). He says that he does not smoke or use illicit drugs. Vital signs include: pulse rate 120/min, respiratory rate 26/min, and blood pressure 100/70 mm Hg. On examination, the patient’s abdomen is diffusely tender. His breath smells like alcohol, with a fruity tinge to it. Bowel sounds are present. No other findings are noted. Fingerstick glucose is 76mg/dL. After the examination, the patient suddenly and spontaneously vomits. Which of the following is the underlying mechanism of the most likely diagnosis in this patient?
A group of scientists is studying the mechanism of action of various pancreatic hormones in rats. The scientists studied hormone A, which is secreted by the β-cells of the pancreas, and found that hormone A binds to a complex dimeric receptor on the cell membrane and exerts its effects via phosphorylation and subsequent downstream signaling that includes dephosphorylation of different intracellular proteins. Now they are studying hormone B, which is secreted by the α-cells and antagonizes the actions of hormone A. Which 2nd messenger system would hormone B utilize to exert its cellular effects?
A 47-year-old woman with chronic epigastric pain comes to the physician because of a 1-month history of intermittent, loose, foul-smelling stools. She has also had a 6-kg (13-lb) weight loss. She has consumed 9–10 alcoholic beverages daily for the past 25 years. Seven years ago, she traveled to Mexico on vacation; she has not been outside the large metropolitan area in which she resides since then. She appears malnourished. The stool is pale and loose; fecal fat content is elevated. An immunoglobulin A serum anti-tissue transglutaminase antibody assay is negative. Further evaluation is most likely to show which of the following?
A 46-year-old man is brought to the emergency department because of severe epigastric pain and vomiting for the past 4 hours. The pain is constant, radiates to his back, and is worse on lying down. He has had 3–4 episodes of greenish-colored vomit. He was treated for H. pylori infection around 2 months ago with triple-regimen therapy. He has atrial fibrillation and hypertension. He owns a distillery on the outskirts of a town. The patient drinks 4–5 alcoholic beverages daily. Current medications include dabigatran and metoprolol. He appears uncomfortable. His temperature is 37.8°C (100°F), pulse is 102/min, and blood pressure is 138/86 mm Hg. Examination shows severe epigastric tenderness to palpation with guarding but no rebound. Bowel sounds are hypoactive. Rectal examination shows no abnormalities. Laboratory studies show: Hematocrit 53% Leukocyte count 11,300/mm3 Serum Na+ 133 mEq/L Cl- 98 mEq/L K+ 3.1 mEq/L Calcium 7.8 mg/dL Urea nitrogen 43 mg/dL Glucose 271 mg/dL Creatinine 2.0 mg/dL Total bilirubin 0.7 mg/dL Alkaline phosphatase 61 U/L AST 19 U/L ALT 17 U/L γ-glutamyl transferase (GGT) 88 u/L (N=5–50 U/L) Lipase 900 U/L (N=14–280 U/L) Which of the following is the most appropriate next step in management?
A 62-year-old Caucasian man visits his primary care provider with recurrent episodes of moderate to severe abdominal pain, nausea, and anorexia for the past 2 years. Additional complaints include constipation, steatorrhea, weight loss, polyphagia, and polyuria. His personal history is relevant for a 2-year period of homelessness when the patient was 55 years old, cigarette smoking since the age of 20, alcohol abuse, and cocaine abuse for which is currently under the supervision of a psychiatry team. He has a pulse of 70/min, a respiratory rate of 16/min, a blood pressure of 130/70 mm Hg, and a body temperature of 36.4°C (97.5°F). His height is 178 cm (5 ft 10 in) and weight is 90 kg (198 lb). On physical examination, he is found to have telangiectasias over the anterior chest, mild epigastric tenderness, and a small nodular liver. Laboratory test results from his previous visit a month ago are shown below: Fasting plasma glucose 160 mg/dL HbA1c 8% Serum triglycerides 145 mg/dL Total cholesterol 250 mg/dL Total bilirubin 0.8 mg/dL Direct bilirubin 0.2 mg/dL Amylase 180 IU/L Lipase 50 IU/L Stool negative for blood; low elastase This patient’s condition is most likely secondary to which of the following conditions?
A 55-year-old man with a history of repeated hospitalization for chronic pancreatitis comes to the physician because of difficulty walking and standing steadily. Neurological examination shows an unsteady, broad-based gait, distal muscle weakness, decreased deep tendon reflexes, and an abnormal Romberg test. His hemoglobin concentration is 11.9 g/dL, mean corpuscular volume is 89/μm3, and serum lactate dehydrogenase is 105 U/L. His serum haptoglobin is slightly decreased. A deficiency of which of the following substances is the most likely cause of this patient's findings?
A 32-year-old man with a history of chronic alcoholism presents to the emergency department with vomiting and diarrhea for 1 week. He states he feels weak and has had poor oral intake during this time. The patient is a current smoker and has presented many times to the emergency department for alcohol intoxication. His temperature is 97.5°F (36.4°C), blood pressure is 102/62 mmHg, pulse is 135/min, respirations are 25/min, and oxygen saturation is 99% on room air. On physical exam, he is found to have orthostatic hypotension and dry mucus membranes. Laboratory studies are ordered as seen below. Serum: Na+: 139 mEq/L Cl-: 101 mEq/L K+: 3.9 mEq/L HCO3-: 25 mEq/L BUN: 20 mg/dL Glucose: 99 mg/dL Creatinine: 1.1 mg/dL Ca2+: 9.8 mg/dL The patient is given normal saline, oral potassium, dextrose, thiamine, and folic acid. The following day, the patient seems confused and complains of diffuse weakness and muscle/bone pain. An ECG and head CT are performed and are unremarkable. Which of the following is the most likely explanation for this patient's new symptoms?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app