
Pancreatitis — MCQs

On this page
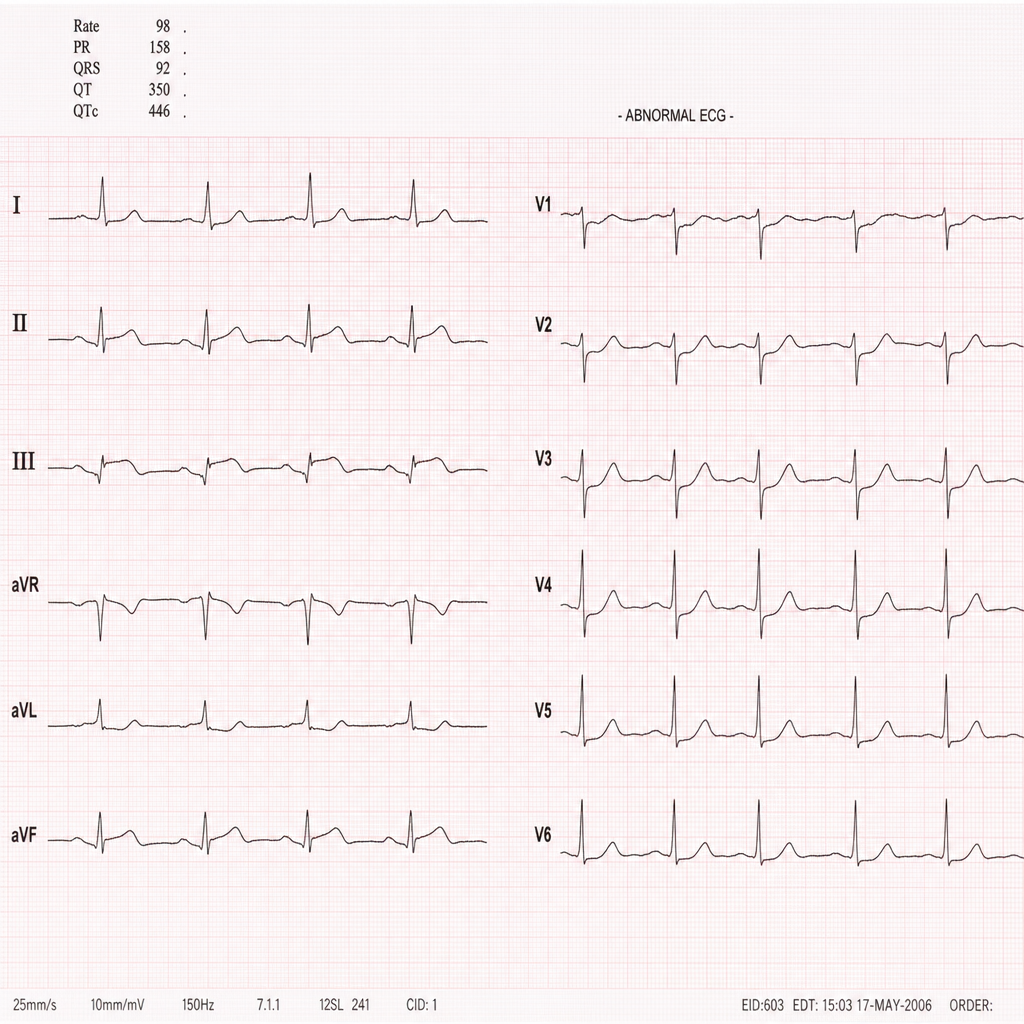
A 68-year-old woman with type 2 diabetes mellitus presents to the emergency department with a 6-hour history of nausea, diaphoresis, and jaw discomfort. She denies chest pain. Her blood pressure is 148/92 mmHg, heart rate is 94 bpm, respiratory rate is 18/min, and oxygen saturation is 97% on room air. An ECG is obtained showing ST elevation in leads II, III, and aVF with reciprocal ST depression in leads I and aVL, consistent with an inferior STEMI. Her troponin I is 3.2 ng/mL (reference <0.04 ng/mL). The catheterization laboratory is available. Which of the following is the most appropriate next step in management?
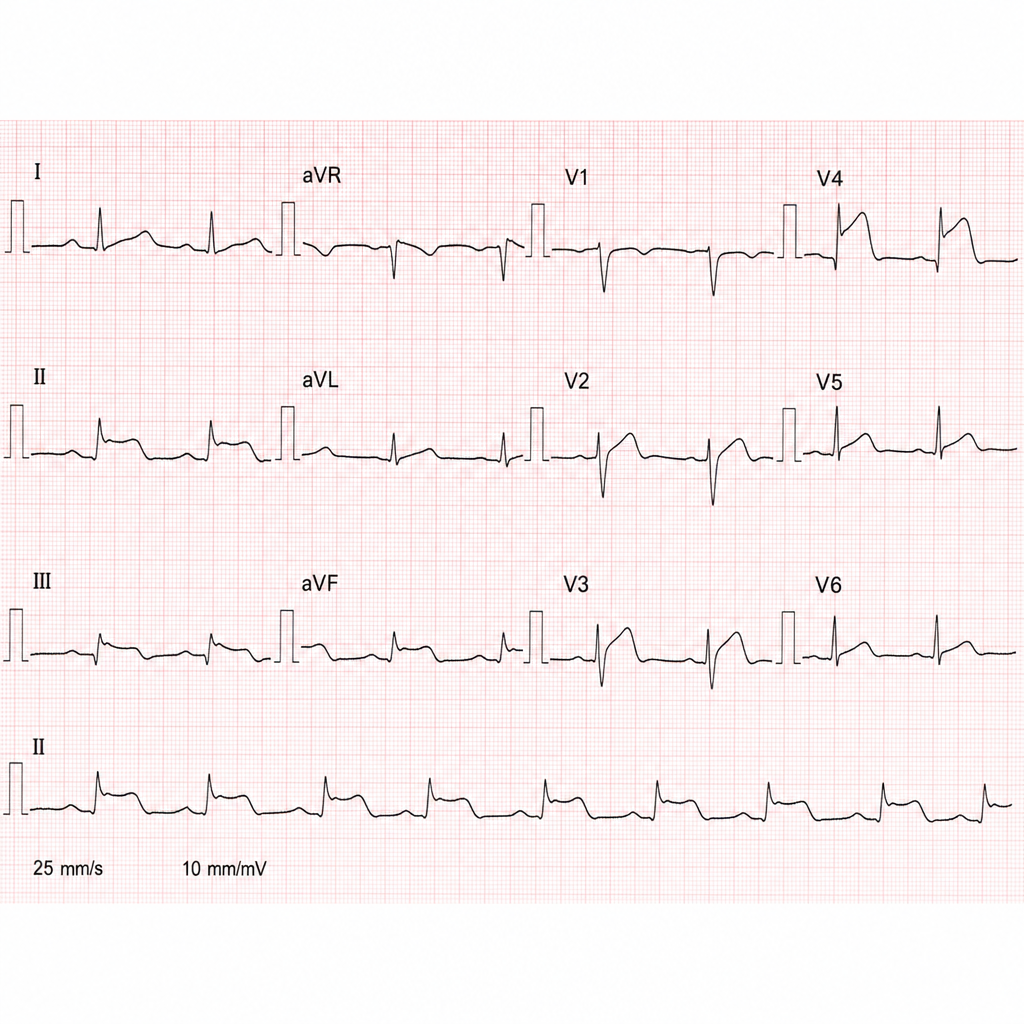
A 67-year-old man with a history of hypertension and type 2 diabetes presents to the emergency department with 2 hours of epigastric discomfort, diaphoresis, and mild dyspnea. He denies chest pain. Vitals: BP 148/92 mmHg, HR 98 bpm, RR 18, SpO2 96% on room air. An ECG shows 2 mm ST elevations in leads II, III, and aVF with reciprocal ST depressions in leads I and aVL. Which of the following is the most appropriate next step in management?
A patient presents with acute epigastric pain and an increase in serum lipase. Several days after stabilization, a chest X-ray shows bilateral diffuse infiltrates. What is the most common pathology explaining the chest X-ray findings?

A 48-year old man comes to the physician for the evaluation of an 8-month history of fatigue and profuse, watery diarrhea. He reports that he has had a 10.5-kg (23-lb) weight loss during this time. Physical examination shows conjunctival pallor and poor skin turgor. Laboratory studies show: Hemoglobin 9.8 g/dl Serum Glucose (fasting) 130 mg/dl K+ 2.5 mEq/L Ca2+ 12 mg/dl A CT scan of the abdomen with contrast shows a 3.0 × 3.2 × 4.4 cm, well-defined, enhancing lesion in the pancreatic tail. Further evaluation of this patient is most likely to show which of the following findings?
A 57-year-old man is admitted to the ER due to an abrupt onset of abdominal pain that radiates to the back, nausea, and multiple vomiting episodes for the past 10 hours. He does not have any significant past medical history. He admits to drinking alcohol every night. During admission, he is found to have a body temperature of 37.5°C (99.5°F), a respiratory rate of 20/min, a pulse of 120/min, and a blood pressure of 120/76 mm Hg. He looks pale with sunken eyes and has significant epigastric tenderness and flank discoloration. An initial laboratory panel shows the following: Total count (WBC) 10,000/mm3 Platelet count 140,000/mm3 Serum glucose 160 mg/dL Serum LDH 500 IU/L Aspartate aminotransferase 400 IU/dL Serum Amylase 500 IU/L Serum Lipase 300 IU/L Which of the following combinations would best predict severity in this case?
An 82-year-old woman presents with 2 months of foul-smelling, greasy diarrhea. She says that she also has felt very tired recently and has had some associated bloating and flatus. She denies any recent abdominal pain, nausea, melena, hematochezia, or vomiting. She also denies any history of recent travel and states that her home has city water. Which of the following tests would be most appropriate to initially work up the most likely diagnosis in this patient?
A 52-year-old woman presents to the urgent care center with several hours of worsening abdominal discomfort with radiation to the back. The patient also complains of malaise, chills, nausea, and vomiting. Social history is notable for alcoholism. On physical exam, she is febrile to 39.5°C (103.1°F), and she is diffusely tender to abdominal palpation. Complete blood count is notable for 13,500 white blood cells, bilirubin 2.1, lipase 842, and amylase 3,210. Given the following options, what is the most likely diagnosis?
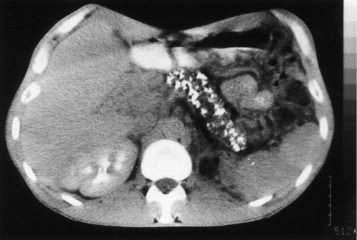
A 42-year-old man comes to the physician because of severe epigastric pain for a week. The pain is constant and he describes it as 6 out of 10 in intensity. The pain radiates to his back and is worse after meals. He has had several episodes of nausea and vomiting during this period. He has taken ibuprofen for multiple similar episodes of pain during the past 6 months. He also has had a 5.4-kg (12-lb) weight loss over the past 4 months. He has a 12-year history of drinking 3 to 4 pints of rum daily. He has been hospitalized three times for severe abdominal pain in the past 3 years. He appears ill. His temperature is 37°C (98.6°F), pulse is 87/min, and blood pressure is 110/70 mm Hg. There is severe epigastric tenderness to palpation. Bowel sounds are normal. Cardiopulmonary examination shows no abnormalities. Laboratory studies show: Hemoglobin 13.6 g/dL Leukocyte count 7,800/mm3 Serum Glucose 106 mg/dL Creatinine 1.1 mg/dL Amylase 150 U/L A CT of the abdomen is shown. Which of the following is the most appropriate long-term management for this patient?
A 59-year-old man presents to the emergency department with diffuse abdominal pain, nausea, and vomiting. Laboratory evaluation on admission is significant for serum glucose of 241 mg/dL, AST of 321 IU/L, and leukocytes of 21,200/μL. Within 3 days of admission with supportive care in the intensive care unit, the patient's clinical condition begins to improve. Based on Ranson's criteria, what is this patient's overall risk of mortality, assuming all other relevant factors are negative?
A 62-year-old Caucasian man visits his primary care provider with recurrent episodes of moderate to severe abdominal pain, nausea, and anorexia for the past 2 years. Additional complaints include constipation, steatorrhea, weight loss, polyphagia, and polyuria. His personal history is relevant for a 2-year period of homelessness when the patient was 55 years old, cigarette smoking since the age of 20, alcohol abuse, and cocaine abuse for which is currently under the supervision of a psychiatry team. He has a pulse of 70/min, a respiratory rate of 16/min, a blood pressure of 130/70 mm Hg, and a body temperature of 36.4°C (97.5°F). His height is 178 cm (5 ft 10 in) and weight is 90 kg (198 lb). On physical examination, he is found to have telangiectasias over the anterior chest, mild epigastric tenderness, and a small nodular liver. Laboratory test results from his previous visit a month ago are shown below: Fasting plasma glucose 160 mg/dL HbA1c 8% Serum triglycerides 145 mg/dL Total cholesterol 250 mg/dL Total bilirubin 0.8 mg/dL Direct bilirubin 0.2 mg/dL Amylase 180 IU/L Lipase 50 IU/L Stool negative for blood; low elastase This patient’s condition is most likely secondary to which of the following conditions?
Practice by Chapter
Acute pancreatitis etiology
Practice Questions
Acute pancreatitis diagnosis
Practice Questions
Severity assessment in acute pancreatitis
Practice Questions
Management of acute pancreatitis
Practice Questions
Local complications of acute pancreatitis
Practice Questions
Systemic complications of acute pancreatitis
Practice Questions
Chronic pancreatitis pathophysiology
Practice Questions
Diagnosis of chronic pancreatitis
Practice Questions
Pain management in chronic pancreatitis
Practice Questions
Exocrine pancreatic insufficiency
Practice Questions
Endocrine complications in pancreatitis
Practice Questions
Autoimmune pancreatitis
Practice Questions
Pancreatic cancer risk in chronic pancreatitis
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app