
Kidney transplantation — MCQs

A 62-year-old female with a history of uncontrolled hypertension undergoes kidney transplantation. One month following surgery she has elevated serum blood urea nitrogen and creatinine and the patient complains of fever and arthralgia. Her medications include tacrolimus and prednisone. If the patient were experiencing acute, cell-mediated rejection, which of the following would you most expect to see upon biopsy of the transplanted kidney?
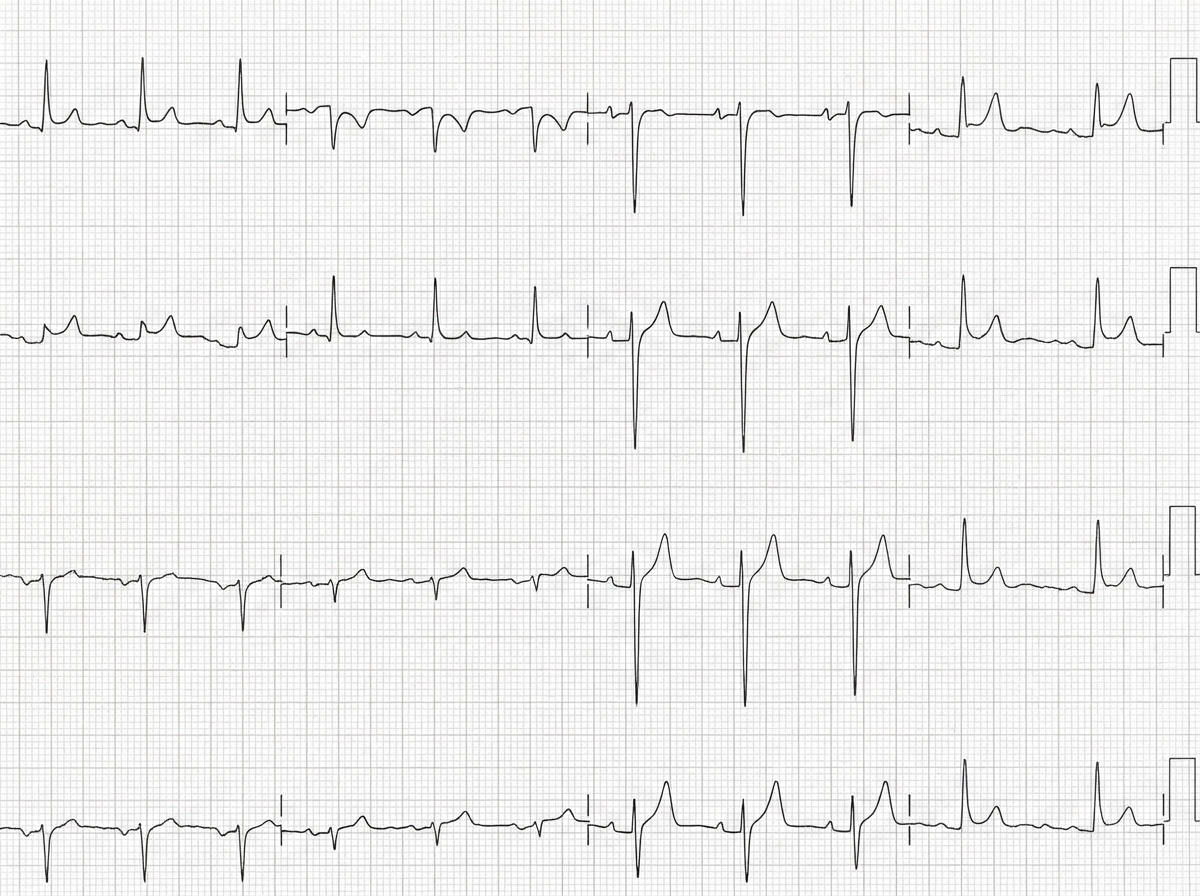
A 50-year-old man with a history of stage 4 kidney disease was admitted to the hospital for an elective hemicolectomy. His past medical history is significant for severe diverticulitis. After the procedure he becomes septic and was placed on broad spectrum antibiotics. On morning rounds, he appear weak and complains of fatigue and nausea. His words are soft and he has difficulty answering questions. His temperature is 38.9°C (102.1°F), heart rate is 110/min, respiratory rate is 15/min, blood pressure 90/65 mm Hg, and saturation is 89% on room air. On physical exam, his mental status appears altered. He has a bruise on his left arm that spontaneously appeared overnight. His cardiac exam is positive for a weak friction rub. Blood specimens are collected and sent for evaluation. An ECG is performed (see image). What therapy will this patient most likely receive next?
Twelve days after undergoing a cadaveric renal transplant for adult polycystic kidney disease, a 23-year-old man has pain in the right lower abdomen and generalized fatigue. During the past 4 days, he has had decreasing urinary output. Creatinine concentration was 2.3 mg/dL on the second postoperative day. Current medications include prednisone, cyclosporine, azathioprine, and enalapril. His temperature is 38°C (100.4°F), pulse is 103/min, and blood pressure is 168/98 mm Hg. Examination reveals tenderness to palpation on the graft site. Creatinine concentration is 4.3 mg/dL. A biopsy of the transplanted kidney shows tubulitis. C4d staining is negative. Which of the following is the most likely cause of this patient's findings?
A 28-year-old woman comes to the physician for a follow-up examination. Two months ago, she underwent left renal transplantation for recurrent glomerulonephritis. At the time of discharge, her creatinine was 0.9 mg/dL. She feels well. Current medications include tacrolimus and azathioprine. Her pulse is 85/min and blood pressure is 135/75 mmHg. Physical examination shows a well-healed surgical scar on her left lower abdomen. The remainder of the examination shows no abnormalities. The patient should be monitored for which of the following adverse effects of her medications?
A 46-year-old man comes to the physician because of a 4-month history of progressively worsening fatigue and loss of appetite. Five years ago, he received a kidney transplant from a living family member. Current medications include sirolimus and mycophenolate. His blood pressure is 150/95 mm Hg. Laboratory studies show normocytic, normochromic anemia and a serum creatinine concentration of 3.1 mg/dL; his vital signs and laboratory studies were normal 6 months ago. Which of the following is the most likely underlying mechanism of this patient’s increase in creatinine concentration?
Several weeks following a kidney transplantation, a 50-year-old Caucasian female presents for evaluation of the transplanted organ. Biopsy shows inflammation involving the endothelial cells of the kidney vasculature and the presence of mononuclear cells in the interstitium. Which cells are most likely responsible for this presentation?
A 14-year-old boy has undergone kidney transplantation due to stage V chronic kidney disease. A pre-transplantation serologic assessment showed that he is negative for past or present HIV infection, viral hepatitis, EBV, and CMV infection. He has a known allergy for macrolides. The patient has no complaints 1 day after transplantation. His vital signs include: blood pressure 120/70 mm Hg, heart rate 89/min, respiratory rate 17/min, and temperature 37.0°C (98.6°F). On physical examination, the patient appears to be pale, his lungs are clear on auscultation, heart sounds are normal, and his abdomen is non-tender on palpation. His creatinine is 0.65 mg/dL (57.5 µmol/L), GFR is 71.3 mL/min/1.73 m2, and urine output is 0.9 mL/kg/h. Which of the following drugs should be used in the immunosuppressive regimen in this patient?
A 58-year-old man is brought to the emergency department because of confusion, weight loss, and anuria. He has chronic kidney disease, hypertension, and type 2 diabetes mellitus. He was diagnosed with acute lymphoblastic leukemia at the age of 8 years and was treated with an allogeneic stem cell transplantation. He is HIV-positive and has active hepatitis C virus infection. He drinks around 8 cans of beer every week. His current medications include tenofovir, emtricitabine, atazanavir, daclatasvir, sofosbuvir, insulin, amlodipine, and enalapril. He appears lethargic. His temperature is 36°C (96.8°F), pulse is 130/min, respirations are 26/min, and blood pressure is 145/90 mm Hg. Examination shows severe edema in his legs and generalized muscular weakness. Auscultation of the lung shows crepitant rales. Laboratory studies show positive HCV antibody and positive HCV RNA. His HIV viral load is undetectable and his CD4+ T-lymphocyte count is 589/μL. Six months ago, his CD4+ T-lymphocyte count was 618/μL. An ECG of the heart shows arrhythmia with frequent premature ventricular contractions. Arterial blood gas analysis on room air shows: pH 7.23 PCO2 31 mm Hg HCO3- 13 mEq/L Base excess -12 mEq/L The patient states he would like to donate organs or tissues in the case of his death. Which of the following is an absolute contraindication for organ donation in this patient?
A 68-year-old woman comes to the physician for a follow-up examination. Three months ago, she underwent heart transplantation for restrictive cardiomyopathy and was started on transplant rejection prophylaxis. Her pulse is 76/min and blood pressure is 148/82 mm Hg. Physical examination shows enlargement of the gum tissue. There is a well-healed scar on her chest. Serum studies show hyperlipidemia. The physician recommends removing a drug that decreases T cell activation by inhibiting the transcription of interleukin-2 from the patient's treatment regimen and replacing it with a different medication. Which of the following drugs is the most likely cause of the adverse effects seen in this patient?
An 18-year-old man is brought to the emergency department due to the confusion that started earlier in the day. His parents report that the patient had recovered from vomiting and diarrhea 3 days ago without medical intervention. They mention that although nausea and vomiting have resolved, the patient continued to have diffuse abdominal pain and decreased appetite. Past medical history is unremarkable, except for a recent weight loss and increased thirst. The patient does not use tobacco products or alcohol. He is not sexually active and does not use illicit drugs. He appears lethargic but responds to questions. His mucous membranes appear dry. Temperature is 36.9°C (98.4°F), blood pressure is 105/60 mm Hg, pulse is 110/min, and respiratory rate is 27/min with deep and rapid respiration. There is diffuse abdominal tenderness without guarding, rebound tenderness or rigidity. Which of the following is the next best step in the management of this patient?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app