
Liver disease — MCQs

On this page
A 46-year-old man comes to the physician for a follow-up examination. Two weeks ago, he underwent laparoscopic herniorrhaphy for an indirect inguinal hernia. During the procedure, a black liver was noted. He has a history of intermittent scleral icterus that resolved without treatment. Serum studies show: Aspartate aminotransferase 30 IU/L Alanine aminotransferase 35 IU/L Alkaline phosphatase 47 mg/dL Total bilirubin 1.7 mg/dL Direct bilirubin 1.1 mg/dL Which of the following is the most likely diagnosis?
A 59-year-old man presents to his primary care physician for fatigue. In general, he has been in good health; however, he recently has experienced some weight loss, abdominal pain, and general fatigue. He has a past medical history of anxiety, diabetes, a fracture of his foot sustained when he tripped, and a recent cold that caused him to miss work for a week. His current medications include metformin, insulin, buspirone, vitamin D, calcium, and sodium docusate. His temperature is 99.5°F (37.5°C), blood pressure is 150/100 mmHg, pulse is 90/min, respirations are 18/min, and oxygen saturation is 98% on room air. Physical exam reveals a calm gentleman. A mild systolic murmur is heard in the left upper sternal region. The rest of the physical exam is within normal limits. Laboratory values are ordered as seen below. Hemoglobin: 12 g/dL Hematocrit: 36% Leukocyte count: 66,500/mm^3 with normal differential Platelet count: 177,000/mm^3 Leukocyte alkaline phosphatase: elevated Serum: Na+: 139 mEq/L Cl-: 100 mEq/L K+: 4.3 mEq/L BUN: 20 mg/dL Glucose: 120 mg/dL Creatinine: 1.1 mg/dL Ca2+: 10.9 mEq/L AST: 12 U/L ALT: 10 U/L Which of the following is the most likely diagnosis?
A 42-year-old woman comes to the physician with a rash on the dorsal surfaces of her hands and feet for the past month. The rash began as blisters that developed a few days after she had been sunbathing on the beach. Photographs of the rash are shown. She has no history of similar symptoms, takes no medications, and has no history of recent travels. She has consumed excess alcohol several times over the past 2 months. Her temperature is 37.1°C (98.8°F). The remainder of the physical examination shows no abnormalities. Laboratory studies show elevated plasma porphyrins, with normal urinary 5-aminolevulinic acid and porphobilinogen. Which of the following is the most appropriate next step in management?

A 30-year-old woman presents to the office with chief complaints of skin pigmentation and fragility of the extensor sides of both hands for a month. The lesions are progressive and are not directly sensitive to light. The patient is otherwise healthy and only uses an oral contraceptive. There is no skin disease or similar skin symptoms in family members. She consumes 1 glass of wine twice a week. Dermatological examination reveals erosions, erythematous macules, pigmentation, and atrophic scarring. Blood analysis reveals elevated CRP (34 mg/L), AST (91 U/L), ALT (141 U/L), and serum ferritin (786 ng/mL compared to the normal value of 350 ng/mL). Her BMI is 21 kg/m2. Urine porphyrin test results are negative. Autoimmune laboratory analysis, hepatic panel, and HIV serology are negative with a normal liver ultrasound. Genetic analysis shows a homozygous missense mutation of the HFE gene. What could be the long-term effect of her condition to her liver?
A 28-year-old man presents to the office with complaints of malaise, anorexia, and vomiting for the past 2 weeks. He also says that his urine is dark. The past medical history is unremarkable. The temperature is 36.8°C (98.2°F), the pulse is 72/min, the blood pressure is 118/63 mm Hg, and the respiratory rate is 15/min. The physical examination reveals a slightly enlarged, tender liver. No edema or spider angiomata are noted. Laboratory testing showed the following: HBsAg Positive IgM anti-HBc < 1:1,000 Anti-HBs Negative HBeAg Positive Anti-HBe Negative HBV DNA 2.65 × 10⁹ IU/L Alpha-fetoprotein 125 ng/mL What is the most likely cause of this patient's condition?
A 44-year-old man with HIV comes to the physician for a routine follow-up examination. He has been noncompliant with his antiretroviral medication regimen for several years. He appears chronically ill and fatigued. CD4+ T-lymphocyte count is 180/mm³ (N ≥ 500). Further evaluation of this patient is most likely to show which of the following findings?
A 55-year-old man presents to the emergency department with hematemesis that started 1 hour ago but has subsided. His past medical history is significant for cirrhosis with known esophageal varices which have been previously banded. His temperature is 97.5°F (36.4°C), blood pressure is 114/64 mmHg, pulse is 130/min, respirations are 12/min, and oxygen saturation is 98% on room air. During the patient's physical exam, he begins vomiting again and his heart rate increases with a worsening blood pressure. He develops mental status changes and on exam he opens his eyes and flexes his arms only to sternal rub and is muttering incoherent words. Which of the following is the most appropriate next step in management?
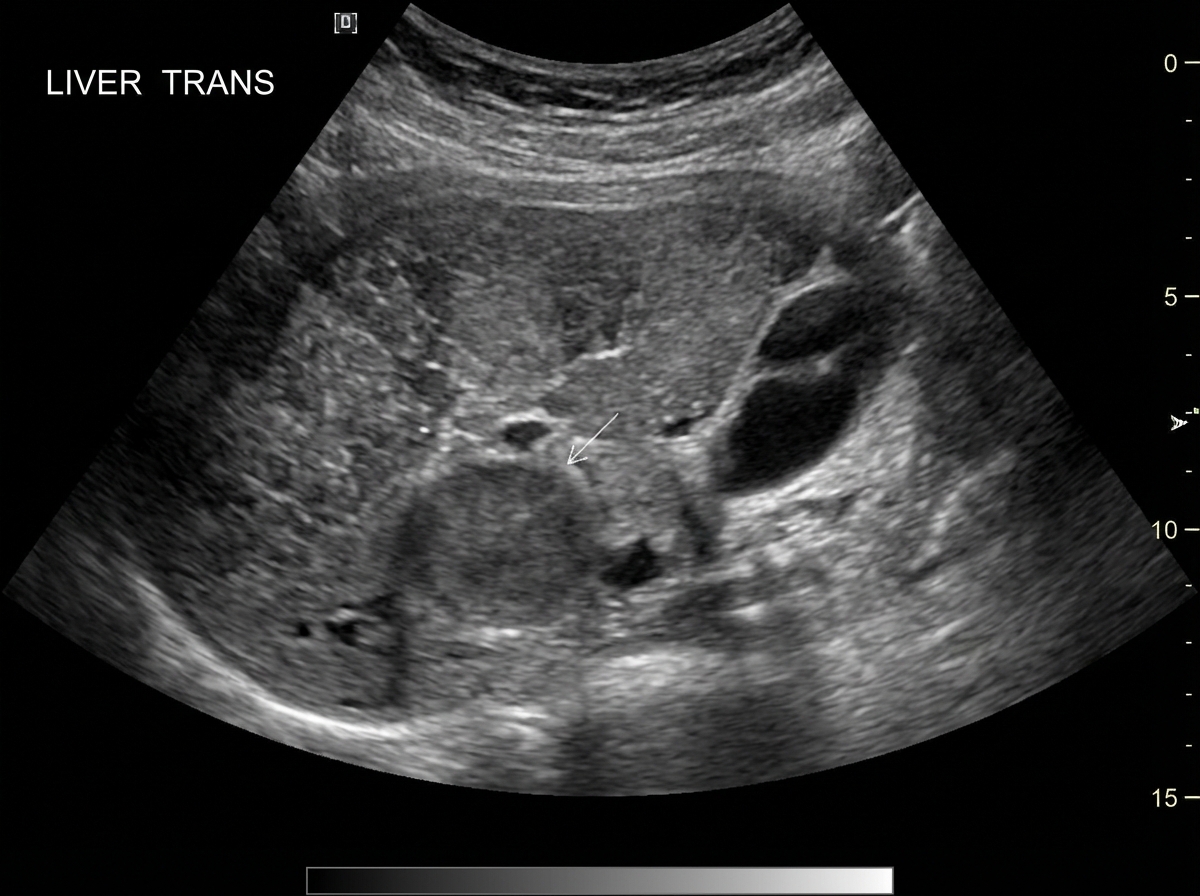
A 61-year-old man comes to the physician because of fatigue and a 5-kg (11-lb) weight loss over the past 6 months. He experimented with intravenous drugs during his 20s and has hepatitis C. His father died of colon cancer. He has smoked one pack of cigarettes daily for 35 years. Physical examination shows scleral icterus and several telangiectasias on the abdomen. The liver is firm and nodular. Laboratory studies show: Hemoglobin 10.9 g/dL Mean corpuscular volume 88 μm3 Leukocyte count 10,400/mm3 Platelet count 260,000/mm3 Ultrasonography of the liver is shown. Which of the following additional findings is most likely?
A 45-year-old man comes to the physician for a routine health maintenance examination. He feels well. He has type 2 diabetes mellitus. There is no family history of serious illness. He works as an engineer at a local company. He does not smoke. He drinks one glass of red wine every other day. He does not use illicit drugs. His only medication is metformin. He is 180 cm (5 ft 11 in) tall and weighs 100 kg (220 lb); BMI is 31 kg/m2. His vital signs are within normal limits. Examination shows a soft, nontender abdomen. The liver is palpated 2 to 3 cm below the right costal margin. Laboratory studies show an aspartate aminotransferase concentration of 100 U/L and an alanine aminotransferase concentration of 130 U/L. Liver biopsy shows hepatocyte ballooning degeneration, as well as inflammatory infiltrates with scattered lymphocytes, neutrophils, and Kupffer cells. Which of the following is the most likely diagnosis?
A 45-year-old man comes to the physician because of a 6-month history of increasing fatigue and reduced libido. He also complains of joint pain in both of his hands. He has a history of hypertension that is controlled with enalapril. He does not smoke or use illicit drugs. He drinks 2–3 beers on the weekends. His vital signs are within normal limits. Physical examination shows a strongly-tanned patient and decreased size of the testes. The second and third metacarpophalangeal joints of both hands are tender to palpation and range of motion is limited. The liver is palpated 2 to 3 cm below the right costal margin. Laboratory studies show: Ferritin 2500 μg/L Aspartate aminotransferase 70 U/L Alanine aminotransferase 80 U/L Glucose 250 mg/dL This patient is at greatest risk for developing which of the following complications?
Practice by Chapter
Viral hepatitis (A, B, C, D, E)
Practice Questions
Alcoholic liver disease
Practice Questions
Non-alcoholic fatty liver disease
Practice Questions
Drug-induced liver injury
Practice Questions
Autoimmune hepatitis
Practice Questions
Cirrhosis management
Practice Questions
Portal hypertension complications
Practice Questions
Ascites diagnosis and management
Practice Questions
Hepatic encephalopathy
Practice Questions
Spontaneous bacterial peritonitis
Practice Questions
Hepatorenal syndrome
Practice Questions
Hepatocellular carcinoma
Practice Questions
Liver transplantation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app