
Liver disease — MCQs

On this page
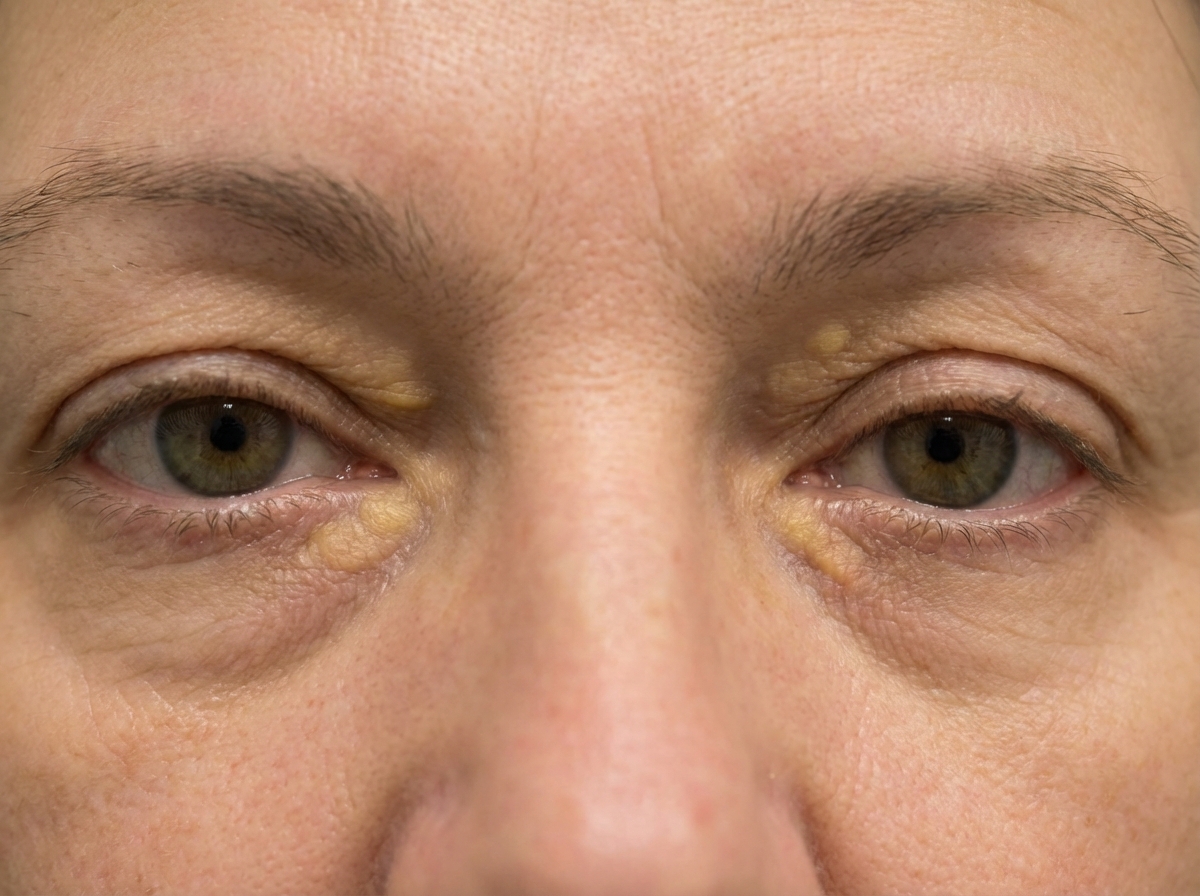
A 57-year-old woman comes to the physician because of a 1-month history of lesions on her eyelids. A photograph of the lesions is shown. This patient's eye condition is most likely associated with which of the following processes?
A 37-year-old woman comes to the office complaining of fatigue and itchiness for the past 2 months. She tried applying body lotion with limited improvement. Her symptoms have worsened over the past month, and she is unable to sleep at night due to intense itching. She feels very tired throughout the day and complains of decreased appetite. She does not smoke cigarettes or drink alcohol. Her past medical history is noncontributory. Her father has diabetes and is on medications, and her mother has hypothyroidism for which she is on thyroid supplementation. Temperature is 36.1°C (97°F), blood pressure is 125/75 mm Hg, pulse is 80/min, respiratory rate is 16/min, and BMI is 25 kg/m2. On examination, her sclera appears icteric. There are excoriations all over her body. Abdominal and cardiopulmonary examinations are negative. Laboratory test Complete blood count Hemoglobin 11.5 g/dL Leukocytes 9,000/mm3 Platelets 150,000/mm3 Serum cholesterol 503 mg/dL Liver function test Serum bilirubin 1.7 mg/dL AST 45 U/L ALT 50 U/L ALP 130 U/L (20–70 U/L) Which of the following findings will favor primary biliary cirrhosis over primary sclerosing cholangitis?
A 54-year-old man presents to the emergency department for fatigue and weight loss. He reports feeling increasingly tired over the last several weeks and has lost seven pounds over the last month. His wife has also noticed a yellowing of the eyes. He endorses mild nausea but denies vomiting, abdominal pain, or changes in his stools. Ten years ago, he was hospitalized for an episode of acute pancreatitis. His past medical history is otherwise significant for hyperlipidemia, diabetes mellitus, and obesity. He has two glasses of wine most nights with dinner and has a 30-pack-year smoking history. On physical exam, the patient has icteric sclera and his abdomen is soft, non-distended, and without tenderness to palpation. Bowel sounds are present. Laboratory studies reveal the following: Alanine aminotransferase (ALT): 67 U/L Aspartate aminotransferase (AST): 54 U/L Alkaline phosphatase: 771 U/L Total bilirubin: 12.1 mg/dL Direct bilirubin: 9.4 mg/dL Which of the following would most likely be seen on abdominal imaging?
A 32-year-old woman comes to the physician with increasing jaundice and fatigue for the past week. She has no history of a serious illness. She takes no medications and denies use of recreational drugs. She does not drink alcohol. Her vital signs are within normal limits. Her body mass index is 21 kg/m2. On physical examination, she has icteric sclera. Otherwise, her heart and lung sounds are within normal limits. Hemoglobin 15 g/dL Leukocyte count 6,000/mm3 with a normal differential Serum bilirubin Total 6.5 mg/dL Direct 0.9 mg/dL Alkaline phosphatase 70 U/L Aspartate aminotransferase (AST, GOT) 430 U/L Alanine aminotransferase (ALT, GPT) 560 U/L γ-Glutamyltransferase (GGT) 43 U/L (N=5-50 U/L) Hepatitis A antibody Negative Hepatitis B surface antigen Negative Hepatitis C antibody Negative Rheumatoid factor 80 IU/mL (N=0-20 IU/mL) Antinuclear antibody (ANA) titer is 1:1280. Polyclonal immunoglobulin gamma is 5 g/dL. Which of the following antibodies is most likely to be positive in this patient?
A 61-year-old woman presents to the emergency department with bloody vomiting for the last hour. She had been vomiting for several hours. Additionally, she states she felt a sudden onset of chest and epigastric pain when she noted blood in her vomit. In the emergency room, she endorses feeling lightheaded and denies difficulty breathing or coughing, and the pain is not worse with swallowing. On review of systems, she notes that she has been bruising more easily than usual over the last 3 months. The patient has a long history of alcoholism with recent progression of liver disease to cirrhosis. She has known esophageal varices and is on propranolol for prophylaxis. In the emergency room, the patient’s temperature is 98.2°F (36.8°C), blood pressure is 94/60 mmHg, pulse is 103/min, and respirations are 16/min. On exam, she is in moderate distress, and there is frank blood in her emesis basin. Cardiovascular and lung exams are unremarkable, and there is pain on palpation of her epigastrium and chest without crepitus. Initial labs are shown below: Hemoglobin: 13.1 g/dL Leukocyte count: 6,200/mm^3 Platelet count: 220,000/mm^3 Creatinine: 0.9 mg/dL The patient is started on IV isotonic saline, pantoprazole, ceftriaxone, and octreotide. Which of the following is the best next step in management?
A 38-year-old man presents with pruritus and jaundice. Past medical history is significant for ulcerative colitis diagnosed 2 years ago, well managed medically. He is vaccinated against hepatitis A and B and denies any recent travel abroad. On physical examination, prominent hepatosplenomegaly is noted. Which of the following would confirm the most likely diagnosis in this patient?
A 44-year-old woman is brought to the emergency department by her husband because of increasing confusion for 3 days. Her husband states that he noticed a yellowish discoloration of her eyes for the past 6 days. She has osteoarthritis. Current medications include acetaminophen and a vitamin supplement. She does not drink alcohol. She uses intravenous cocaine occasionally. She appears ill. Her temperature is 37.2 °C (99.0 °F), pulse is 102/min, respirations are 20/min, and blood pressure is 128/82 mm Hg. She is confused and oriented only to person. Examination shows scleral icterus and jaundice of her skin. Flapping tremors of the hand when the wrist is extended are present. The liver edge is palpated 4 cm below the right costal margin and is tender; there is no splenomegaly. Hemoglobin 12.4 g/dL Leukocyte count 13,500/mm3 Platelet count 100,000/mm3 Prothrombin time 68 sec (INR=4.58) Serum Na+ 133 mEq/L Cl- 103 mEq/L K+ 3.6 mEq/L Urea nitrogen 37 mg/dL Glucose 109 mg/dL Creatinine 1.2 mg/dL Total bilirubin 19.6 mg/dL AST 1356 U/L ALT 1853 U/L Hepatitis B surface antigen positive Hepatitis B surface antibody negative Hepatitis C antibody negative Anti-hepatitis A virus IgM negative Acetaminophen level 12 mcg/mL (N < 20 mcg/mL) The patient is transferred to the intensive care unit and treatment with tenofovir is begun. Which of the following is the most appropriate next step in the management of this patient?
A 70-year-old man without recent travel history presents with a 2-week history of gradually worsening generalized pruritus. He is unsure if his skin has yellowed, and carries an identification card without a photograph for comparison. On physical examination, the liver morphology is normal. A basic chemistry panel reveals sodium 139 mmol/L, potassium 3.8 mmol/L, chloride 110 mmol/L, carbon dioxide 27, blood urea nitrogen 26 mg/dL, creatinine 0.84 mg/dL, and glucose 108 mg/dL. Which of the following is the least compatible with the patient's provided history?
A 73-year-old woman visits an urgent care clinic with a complaint of fever for the past 48 hours. She has been having frequent chills and increasing abdominal pain since her fever spiked to 39.4°C (103.0°F) at home. She states that abdominal pain is constant, non-radiating, and rates the pain as a 4/10. She also complains of malaise and fatigue. The past medical history is insignificant. The vital signs include: heart rate 110/min, respiratory rate 15/min, temperature 39.2°C (102.5°F), and blood pressure 120/86 mm Hg. On physical examination, she is icteric and there is severe tenderness on palpation of the right hypochondrium. The ultrasound of the abdomen shows a dilated bile duct and calculus in the bile duct. The blood cultures are pending, and the antibiotic therapy is started. What is the most likely cause of her symptoms?
A 44-year-old man comes to the physician for a routine health maintenance examination. He had not seen his primary care physician for 7 years. He has no complaints other than feeling easily fatigued. He has no significant medical history. He reports drinking half a pint of liquor a day. His temperature is 98.7°F (37.1°C), pulse is 65/min, respiratory rate is 15/min, and blood pressure is 120/70 mm Hg. Physical examination shows reddish color to both of his palms. His abdomen has no focal tenderness but is difficult to assess due to distention. Laboratory studies show: Hemoglobin 11.0 g/dL Hematocrit 33% Leukocyte count 5,000/mm3 Platelet count 60,000/mm3 Serum Na+ 135 mEq/L K+ 4.5 mEq/L Cl- 100 mEq/L HCO3- 24 mEq/L Urea nitrogen 15 mg/dL Creatinine 1.3 mg/dL Total bilirubin 3.0 mg/dL AST 112 U/L ALT 80 U/L Alkaline phosphatase 130 U/L Which of the following is the most likely explanation for this patient's thrombocytopenia?
Practice by Chapter
Viral hepatitis (A, B, C, D, E)
Practice Questions
Alcoholic liver disease
Practice Questions
Non-alcoholic fatty liver disease
Practice Questions
Drug-induced liver injury
Practice Questions
Autoimmune hepatitis
Practice Questions
Cirrhosis management
Practice Questions
Portal hypertension complications
Practice Questions
Ascites diagnosis and management
Practice Questions
Hepatic encephalopathy
Practice Questions
Spontaneous bacterial peritonitis
Practice Questions
Hepatorenal syndrome
Practice Questions
Hepatocellular carcinoma
Practice Questions
Liver transplantation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app