
Liver disease — MCQs

On this page
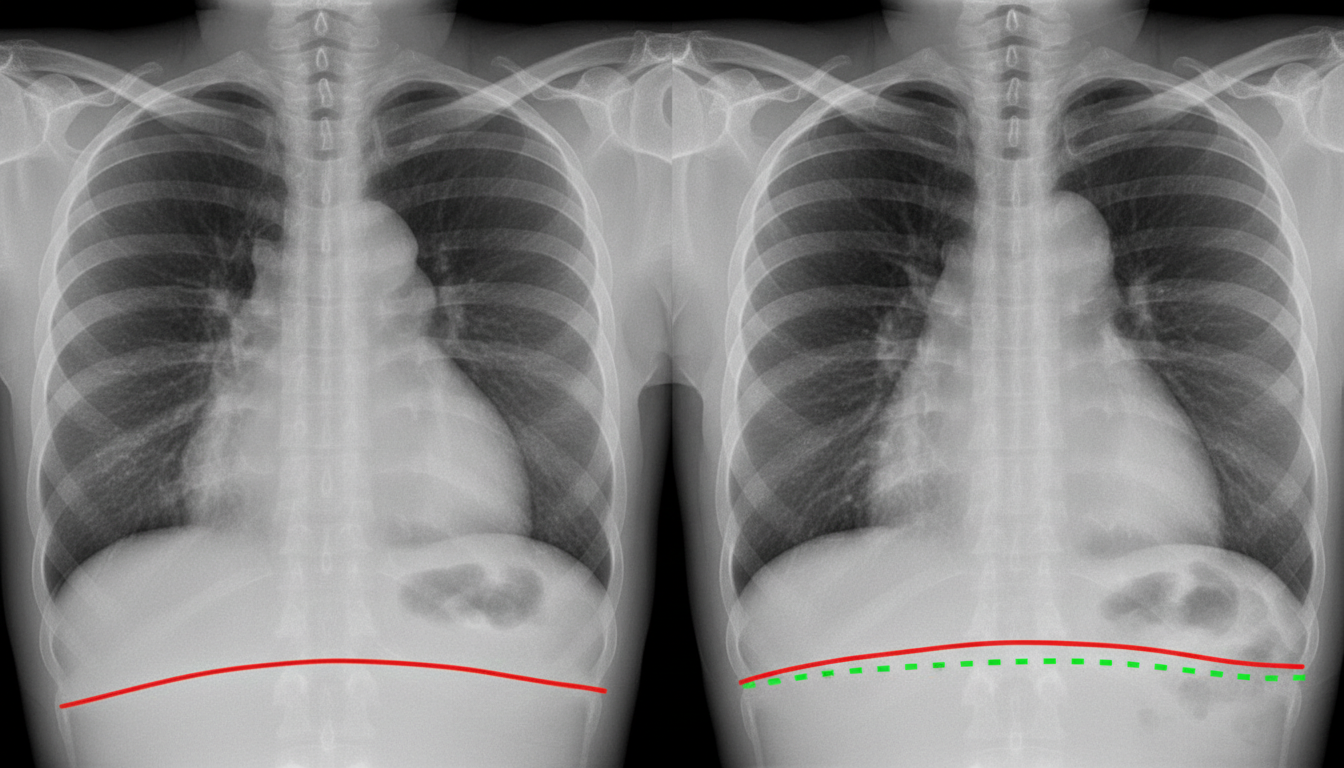
A 28-year-old patient presents to the hospital complaining of progressively worsening dyspnea and a dry cough. Radiographic imaging is shown below. Pulmonary function testing (PFT's) reveals a decreased FEV1 and FEV1/FVC, but an increased TLC. Bronchodilator reversibility testing shows no significant improvement in FEV1 after administration of a bronchodilator. The patient states that he does not smoke. Which of the following conditions is most consistent with the patient's symptoms?
A 44-year-old woman presents to the emergency department with jaundice and diffuse abdominal pain. She denies any previous medical problems and says she does not take any medications, drugs, or supplements. Her temperature is 97.6°F (36.4°C), blood pressure is 133/87 mmHg, pulse is 86/min, respirations are 22/min, and oxygen saturation is 100% on room air. Physical exam is notable for sclera which are icteric and there is tenderness to palpation over the right upper quadrant. Laboratory studies are ordered as seen below. Hepatitis B surface antigen: Positive Hepatitis B surface antibody: Negative Hepatitis B core antibody IgM: Negative Hepatitis B core antibody IgG: Positive Hepatitis B E antigen: Positive Hepatitis B E antibody (anti-HBe): Negative Which of the following is the most likely diagnosis?
A 22-year-old student presents to the college health clinic with a 1-week history of fever, sore throat, nausea, and fatigue. He could hardly get out of bed this morning. There are no pets at home. He admits to having recent unprotected sex. The vital signs include: temperature 38.3°C (101.0°F), pulse 72/min, blood pressure 118/63 mm Hg, and respiratory rate 15/min. On physical examination, he has bilateral posterior cervical lymphadenopathy, exudates over the palatine tonsil walls with soft palate petechiae, an erythematous macular rash on the trunk and arms, and mild hepatosplenomegaly. What is the most likely diagnosis?
A 45-year-old man is brought to the physician for a follow-up examination. Three weeks ago, he was hospitalized and treated for spontaneous bacterial peritonitis. He has alcoholic liver cirrhosis and hypothyroidism. His current medications include spironolactone, lactulose, levothyroxine, trimethoprim-sulfamethoxazole, and furosemide. He appears ill. His temperature is 36.8°C (98.2°F), pulse is 77/min, and blood pressure is 106/68 mm Hg. He is oriented to place and person only. Examination shows scleral icterus and jaundice. There is 3+ pedal edema and reddening of the palms bilaterally. Breast tissue appears enlarged, and several telangiectasias are visible over the chest and back. Abdominal examination shows dilated tortuous veins. On percussion of the abdomen, the fluid-air level shifts when the patient moves from lying supine to right lateral decubitus. Breath sounds are decreased over both lung bases. Cardiac examination shows no abnormalities. Bilateral tremor is seen when the wrists are extended. Genital examination shows reduced testicular volume of both testes. Digital rectal examination and proctoscopy show hemorrhoids. Which of the following potential complications of this patient's condition is the best indication for the placement of a transjugular intrahepatic portosystemic shunt (TIPS)?
A 54-year-old man presents to the emergency department after vomiting blood an hour ago. He says this happens to him occasionally but denies feeling pain in these episodes. The man is disheveled and has slurred speech as he describes his symptoms. He is reluctant to give further history and wants immediate treatment of his condition. Upon examination, the patient has evidence of tortuous veins visible on his abdomen plus a yellow tinge to his sclerae. He suddenly begins vomiting copious amounts of blood and soon becomes unresponsive. His blood pressure drops to 70/40 mm Hg. He is given 3 units of whole blood but passes away shortly after the incident. Which of the following was the most likely cause of his vomiting of blood?
A 33-year-old woman comes to the physician for a follow-up examination. She was treated for a urinary stone 1 year ago with medical expulsive therapy. There is no personal or family history of serious illness. Her only medication is an oral contraceptive pill that she has been taking for 12 years. She appears healthy. Physical examination shows no abnormalities. A complete blood count, serum creatinine, and electrolytes are within the reference range. Urinalysis is within normal limits. An ultrasound of the abdomen shows a well-demarcated hyperechoic 3-cm (1.2-in) hepatic lesion. A contrast-enhanced CT of the abdomen shows a well-demarcated 3-cm hepatic lesion with peripheral enhancement and subsequent centripetal flow followed by rapid clearance of contrast. There is no hypoattenuating central scar. In addition to stopping the oral contraceptive pill, which of the following is the most appropriate next step in management?
A 19-year-old man comes to the physician because of recurrent yellowing of his eyes over the past 2 years. He reports that each episode lasts 1–2 weeks and resolves spontaneously. He has no family history of serious illness. He recently spent a week in Mexico for a vacation. He is sexually active with two partners and uses condoms inconsistently. He does not drink alcohol or use illicit drugs. His vital signs are within normal limits. Physical examination shows jaundice of the conjunctivae and the skin. The abdomen is soft with no organomegaly. The remainder of the physical examination shows no abnormalities. Laboratory studies show: Serum Total bilirubin 4.0 mg/dL Direct bilirubin 3.0 mg/dL Alkaline phosphatase 75 U/L AST 12 U/L ALT 12 U/L Anti-HAV IgG positive HBsAg negative Anti-HBsAg positive HCV RNA negative Urine Bilirubin present Urobilinogen normal Which of the following is the most likely underlying cause of this patient's condition?
A 58-year-old man with a history of hepatitis C presents with unintentional weight loss, weakness, jaundice, splenomegaly, and caput medusae. Which of the following is the most appropriate initial test to assess the degree of hepatocellular injury?
A 32-year-old woman visits the office with a complaint of recurrent abdominal pain for the past 2 months. She says the pain has been increasing every day and is located in the right upper quadrant. She has been using oral contraceptive pills for the past 2 years. She is a nonsmoker and does not drink alcohol. Her vital signs show a heart rate of 85/min, respiratory rate of 16/min, temperature of 37.6 °C (99.68 °F), and blood pressure of 120/80 mm Hg. Physical examination reveals right upper quadrant tenderness and hepatomegaly 3 cm below the right costal border. Her serology tests for viral hepatitis are as follows: HBsAg Negative Anti-HBs Negative IgM anti-HBc Negative Anti-HCV Negative A hepatic ultrasound shows hepatomegaly with diffusely increased echogenicity and a well-defined, predominantly hypoechoic mass in segment VI of the right lobe of the liver. What is the most likely diagnosis?
A 47-year-old man with alcoholic cirrhosis comes to the physician for a follow-up examination. Examination of the skin shows erythema over the thenar and hypothenar eminences of both hands. He also has numerous blanching lesions over the trunk and upper extremities that have a central red vessel with thin extensions radiating outwards. Which of the following is the most likely underlying cause of these findings?
Practice by Chapter
Viral hepatitis (A, B, C, D, E)
Practice Questions
Alcoholic liver disease
Practice Questions
Non-alcoholic fatty liver disease
Practice Questions
Drug-induced liver injury
Practice Questions
Autoimmune hepatitis
Practice Questions
Cirrhosis management
Practice Questions
Portal hypertension complications
Practice Questions
Ascites diagnosis and management
Practice Questions
Hepatic encephalopathy
Practice Questions
Spontaneous bacterial peritonitis
Practice Questions
Hepatorenal syndrome
Practice Questions
Hepatocellular carcinoma
Practice Questions
Liver transplantation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app