
Liver disease — MCQs

On this page
A 45-year-old man comes to the physician because of fatigue and joint pain for 8 months. He has pain in both knees, both elbows, and diffuse muscle pain. He does not have dyspnea. He also had several episodes of a nonpruritic rash on his lower extremities. Eight years ago, the patient was diagnosed with hepatitis C. His temperature is 37.9°C (100.2°F), pulse is 90/min, and blood pressure is 140/90 mm Hg. Examination of the lower extremities shows raised purple papules that do not blanch when pressure is applied. Cardiopulmonary examination shows no abnormalities. Laboratory studies show: Hemoglobin 13.9 g/dL Leukocyte count 8,500/mm3 Platelets 160,000/mm3 Serum Creatinine 1.1 mg/dL ALT 123 U/L AST 113 U/L Further evaluation of this patient is most likely to show which of the following findings?
A 61-year-old man presents to the primary care clinic to establish care. He has not seen a physician for many years. He has no complaints or concerns but, on further questioning, does have some vague abdominal discomfort. He has no known past medical history and takes no medications. His social history is notable for injecting heroin throughout his late-teens and 20s, but he has been clean and sober for over a decade. At the clinic, the vital signs include: heart rate 90/min, respiratory rate 17/min, blood pressure 110/65 mm Hg, and temperature 37.0°C (98.6°F). The physical exam shows a slightly distended abdomen. The laboratory studies are notable for a platelet count of 77,000/uL and an international normalized ratio (INR) of 1.7. Which of the following is the next best step in the diagnosis of this patient?
A 65-year-old man comes to the physician because of progressive abdominal distension and swelling of his legs for 4 months. He has a history of ulcerative colitis. Physical examination shows jaundice. Abdominal examination shows shifting dullness and dilated veins in the periumbilical region. This patient's abdominal findings are most likely caused by increased blood flow in which of the following vessels?
A 25-year-old man presents to the office for a 3-day history of fever and fatigue. Upon further questioning, he says that he also had constant muscular pain, headaches, and fever during these days. He adds additional information by giving a history of regular unprotected sexual relationship with multiple partners. He is a non-smoker and drinks alcohol occasionally. The heart rate is 102/min, respiratory rate is 18/min, temperature is 38.0°C (100.4°F), and blood pressure is 120/80 mm Hg. On physical examination, he is icteric and hepatosplenomegaly is evident with diffuse muscular and abdominal tenderness particularly in the right upper quadrant. The serologic markers show the following pattern: Anti-HAV IgM negative HBsAg positive Anti-HBs negative IgM anti-HBc positive Anti-HCV negative Anti-HDV negative What is the most likely diagnosis?
A 35-year-old man presents with erectile dysfunction. Past medical history is significant for diabetes mellitus diagnosed 5 years ago, managed with insulin, and for donating blood 6 months ago. The patient denies any history of smoking or alcohol use. He is afebrile, and his vital signs are within normal limits. Physical examination shows a bronze-colored hyperpigmentation on the dorsal side of the arms bilaterally. Nocturnal penile tumescence is negative. Routine basic laboratory tests are significant for a moderate increase in glycosylated hemoglobin and hepatic enzymes. Which of the following is the most likely diagnosis in this patient?
A 46-year-old man comes to the clinic complaining of abdominal pain for the past month. The pain comes and goes and is the most prominent after meals. He reports 1-2 episodes of black stools in the past month, a 10-lbs weight loss, fevers, and a skin rash on his left arm. A review of systems is negative for any recent travel, abnormal ingestion, palpitations, nausea/vomiting, diarrhea, or constipation. Family history is significant for a cousin who had liver failure in his forties. His past medical history is unremarkable. He is sexually active with multiple partners and uses condoms intermittently. He admits to 1-2 drinks every month and used to smoke socially during his teenage years. His laboratory values are shown below: Serum: Na+: 138 mEq/L Cl-: 98 mEq/L K+: 3.8 mEq/L HCO3-: 26 mEq/L BUN: 10 mg/dL Glucose: 140 mg/dL Creatinine: 2.1 mg/dL Thyroid-stimulating hormone: 3.5 µU/mL Ca2+: 10 mg/dL AST: 53 U/L ALT: 35 U/L HBsAg: Positive Anti-HBc: Positive IgM anti-HBc: Positive Anti-HBs: Negative What findings would you expect to find in this patient?
A 54-year-old man with known end-stage liver disease from alcoholic cirrhosis presents to the emergency department with decreased urinary output and swelling in his lower extremities. His disease has been complicated by ascites and hepatic encephalopathy in the past. Initial laboratory studies show a creatinine of 1.73 mg/dL up from a previous value of 1.12 one month prior. There have been no new medication changes, and no recent procedures performed. A diagnostic paracentesis is performed that is negative for infection, and he is admitted to the hospital for further management and initiated on albumin. Two days later, his creatinine has risen to 2.34 and he is oliguric. Which of the following is the most definitive treatment for this patient's condition?
A 62-year-old man is brought to the emergency department for the evaluation of intermittent bloody vomiting for the past 2 hours. He has had similar episodes during the last 6 months that usually stop spontaneously within an hour. The patient is not aware of any medical problems. He has smoked one pack of cigarettes daily for 30 years but quit 10 years ago. He drinks half a liter of vodka daily. He appears pale and diaphoretic. His temperature is 37.3°C (99.1°F), pulse is 100/min, respirations are 20/min, and blood pressure is 105/68 mm Hg. Cardiac examination shows no murmurs, rubs, or gallops. There is increased abdominal girth. On percussion of the abdomen, the fluid-air level shifts when the patient moves from the supine to the right lateral decubitus position. The edge of the liver is palpated 2 cm below the costal margin. His hemoglobin concentration is 10.3 g/dL, leukocyte count is 4,200/mm3, and platelet count is 124,000/mm3. Intravenous fluids and octreotide are started. Which of the following is the most appropriate next step in the management of this patient?
A 47-year-old man is brought to the emergency department by police. He was forcibly removed from a bar for lewd behavior. The patient smells of alcohol, and his speech is slurred and unintelligible. The patient has a past medical history of alcohol abuse, obesity, diabetes, and Wernicke encephalopathy. The patient's currently prescribed medications include insulin, metformin, disulfiram, atorvastatin, a multi-B-vitamin, and lisinopril; however, he is non-compliant with his medications. His temperature is 98.5°F (36.7°C), blood pressure is 150/97 mmHg, pulse is 100/min, respirations are 15/min, and oxygen saturation is 96% on room air. Physical exam is notable for a palpable liver edge 2 cm inferior to the rib cage and increased abdominal girth with a positive fluid wave. Laboratory values are ordered and return as below: Hemoglobin: 10 g/dL Hematocrit: 33% Leukocyte count: 7,500 cells/mm^3 with normal differential Platelet count: 245,000/mm^3 Serum: Na+: 136 mEq/L Cl-: 102 mEq/L K+: 4.1 mEq/L HCO3-: 24 mEq/L BUN: 24 mg/dL Glucose: 157 mg/dL Creatinine: 1.5 mg/dL Ca2+: 9.6 mg/dL Which of the following are the most likely laboratory values that would be seen in this patient in terms of aspartate aminotransferase (AST), alanine aminotransferase (ALT) and gamma-glutamyl transferase (GGT) (in U/L)?
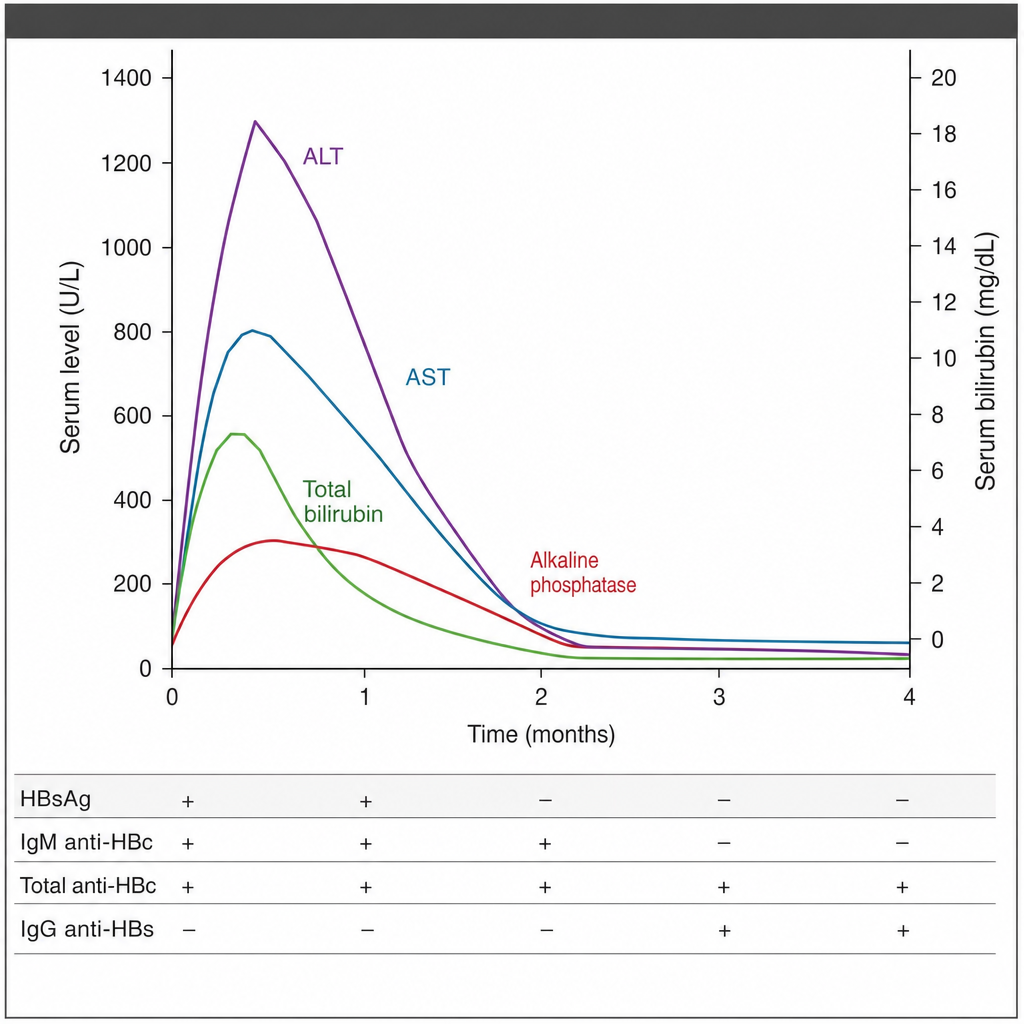
A 37-year-old man comes to the physician because of a 3-day history of fatigue and yellowish discoloration of his eyes and skin. Physical examination shows mild right upper quadrant abdominal tenderness. The course of different serum parameters over the following 4 months is shown. Which of the following is the most likely explanation for the course of this patient's laboratory findings?
Practice by Chapter
Viral hepatitis (A, B, C, D, E)
Practice Questions
Alcoholic liver disease
Practice Questions
Non-alcoholic fatty liver disease
Practice Questions
Drug-induced liver injury
Practice Questions
Autoimmune hepatitis
Practice Questions
Cirrhosis management
Practice Questions
Portal hypertension complications
Practice Questions
Ascites diagnosis and management
Practice Questions
Hepatic encephalopathy
Practice Questions
Spontaneous bacterial peritonitis
Practice Questions
Hepatorenal syndrome
Practice Questions
Hepatocellular carcinoma
Practice Questions
Liver transplantation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app