
Liver disease — MCQs

On this page
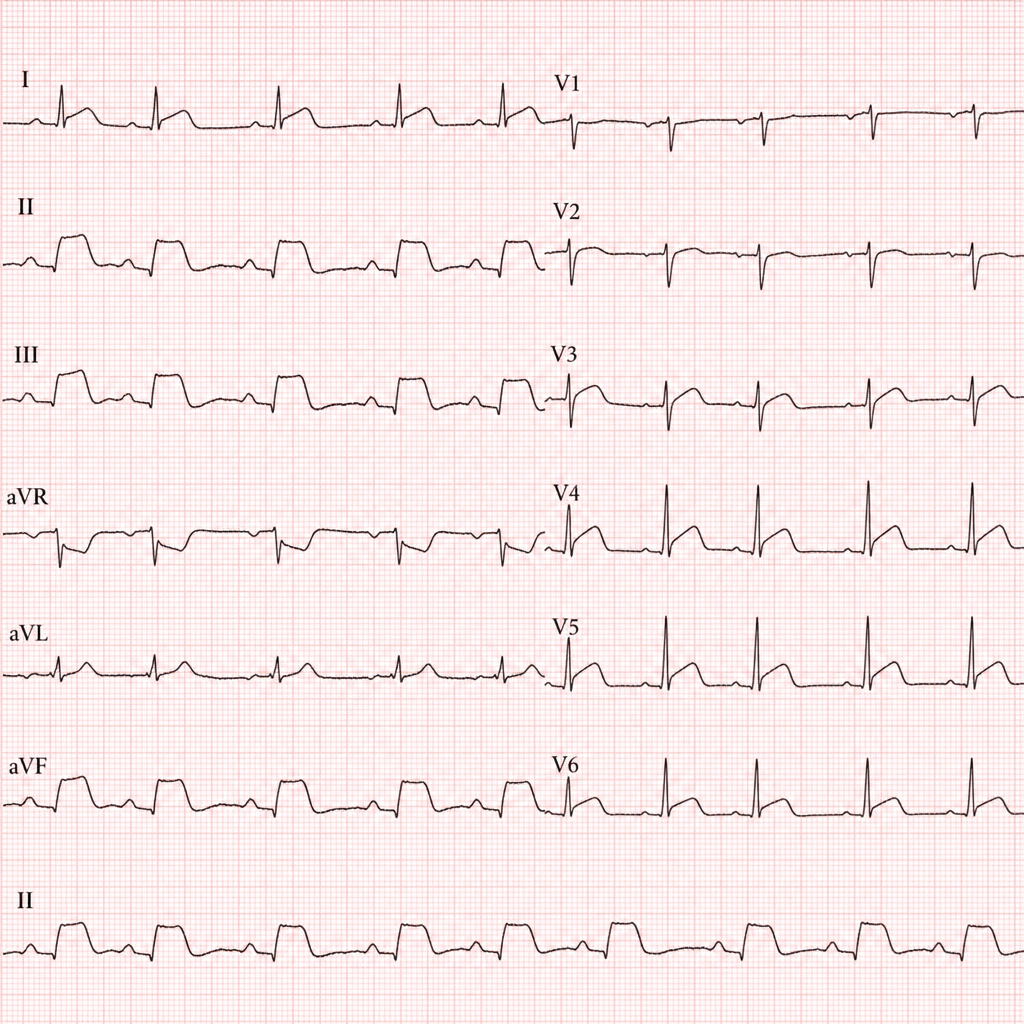
A 68-year-old woman with a history of hypertension and type 2 diabetes presents to the emergency department with 3 hours of epigastric discomfort, nausea, and diaphoresis. She denies chest pain or dyspnea. Her blood pressure is 148/92 mmHg, heart rate is 94 bpm, respiratory rate is 18/min, and oxygen saturation is 97% on room air. The ECG demonstrates 2 mm ST-segment elevations in leads II, III, and aVF with reciprocal ST depressions in leads I and aVL. Troponin I is pending. Which of the following is the most appropriate immediate next step in management?
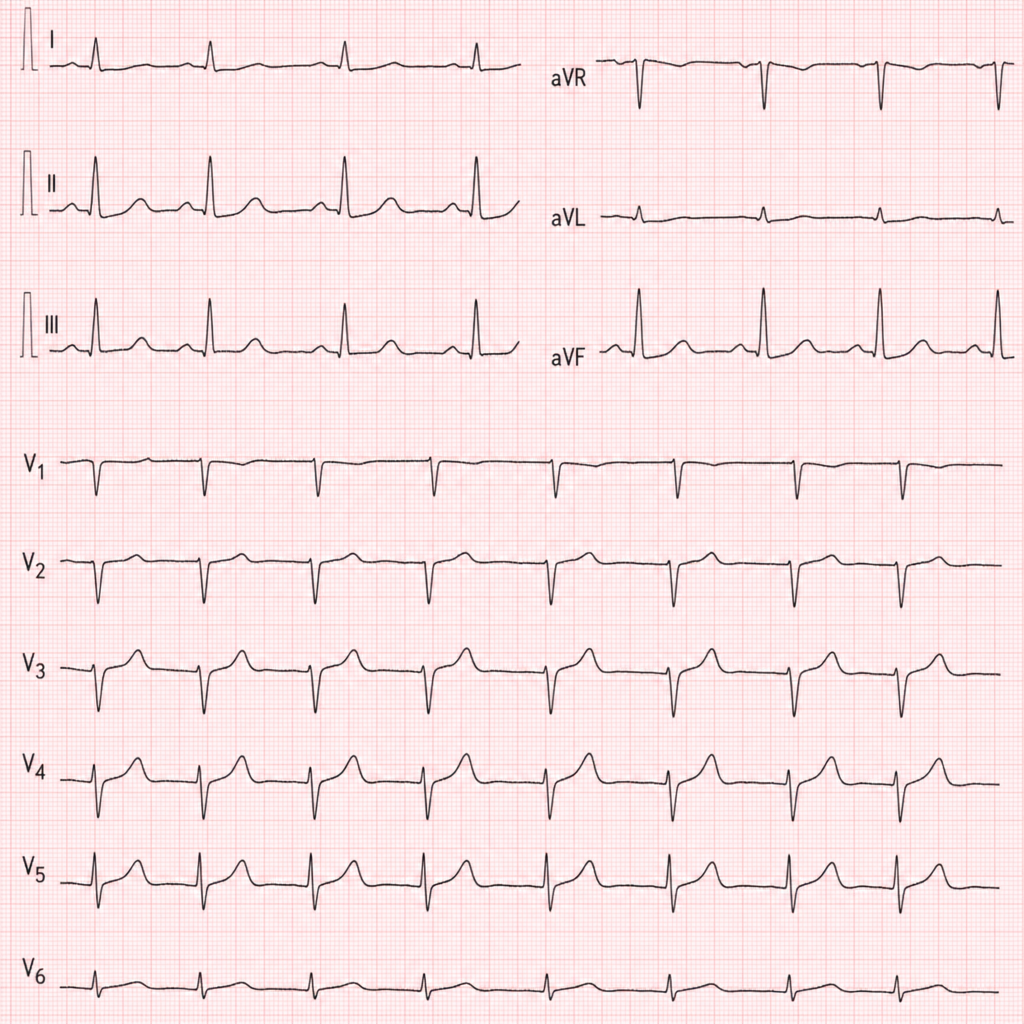
A 67-year-old woman with a history of type 2 diabetes mellitus and hypertension presents to the emergency department with 3 hours of epigastric discomfort, nausea, and diaphoresis. She denies chest pain or shortness of breath. Her blood pressure is 148/92 mmHg, heart rate is 96 bpm, and oxygen saturation is 97% on room air. An ECG is performed showing ST elevations in leads II, III, and aVF. Which of the following is the most appropriate next step in management?
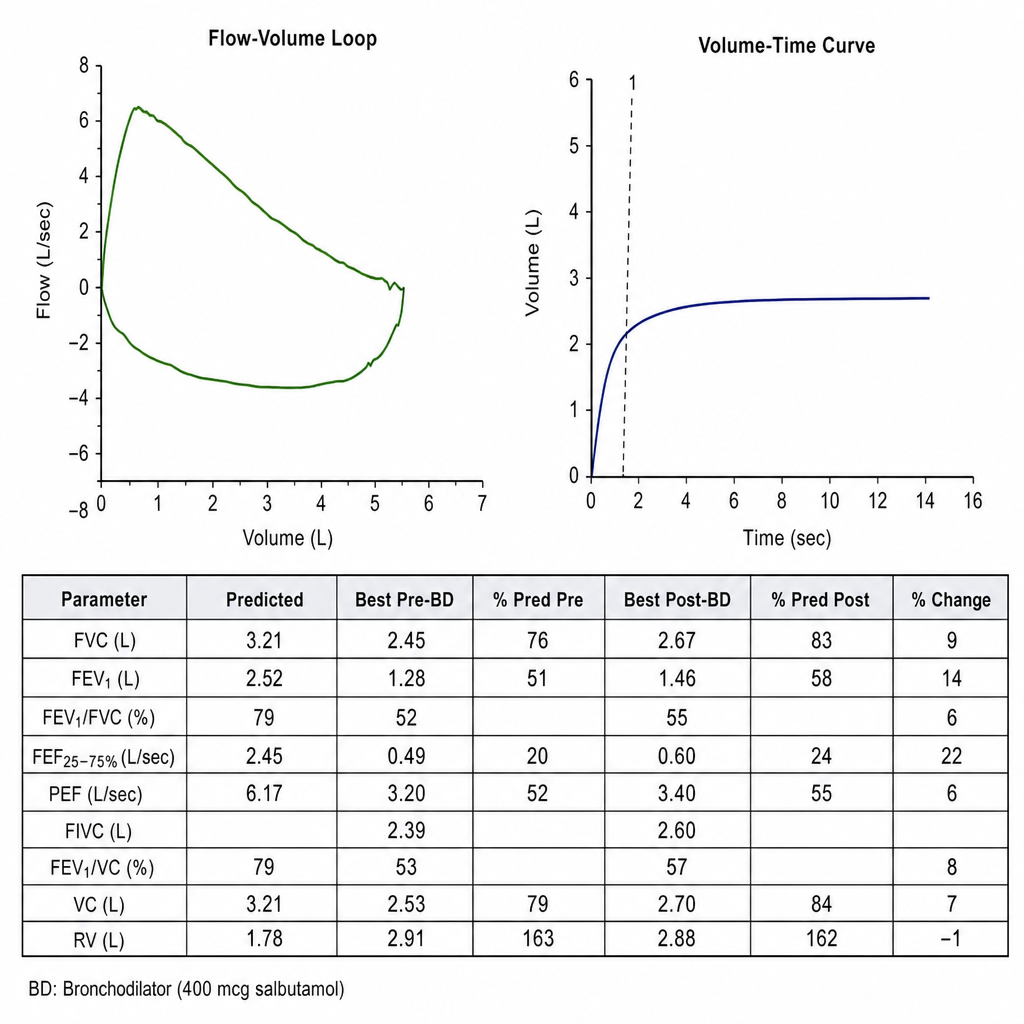
A 54-year-old woman with a 30-pack-year smoking history presents with progressive dyspnea on exertion over 8 months and a chronic productive cough. She reports that her breathlessness limits her to walking on level ground at her own pace and she must stop after about 100 yards due to dyspnea (mMRC grade 2). She has had one exacerbation requiring a course of oral antibiotics in the past year. She denies fever, hemoptysis, or weight loss. Vital signs are normal. Spirometry is performed. Her post-bronchodilator FEV₁/FVC ratio is 0.58 and FEV₁ is 52% of predicted. She is currently using only a short-acting beta-agonist as needed. Which of the following is the most appropriate addition to her maintenance therapy?
A person with a history of chronic alcohol consumption who indulged in binge drinking 10 days ago is brought to the emergency department in an unconscious state. A non-contrast CT scan was normal, and his blood glucose level is 45 mg/dL. What is the most appropriate treatment?
A 40-year-old farmer presents with fever, calf tenderness, conjunctival suffusion, retro-orbital pain, and hypokalemia. What is the diagnosis?
Practice by Chapter
Viral hepatitis (A, B, C, D, E)
Practice Questions
Alcoholic liver disease
Practice Questions
Non-alcoholic fatty liver disease
Practice Questions
Drug-induced liver injury
Practice Questions
Autoimmune hepatitis
Practice Questions
Cirrhosis management
Practice Questions
Portal hypertension complications
Practice Questions
Ascites diagnosis and management
Practice Questions
Hepatic encephalopathy
Practice Questions
Spontaneous bacterial peritonitis
Practice Questions
Hepatorenal syndrome
Practice Questions
Hepatocellular carcinoma
Practice Questions
Liver transplantation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app