
Opportunistic infections — MCQs

For which of the following patients would you recommend prophylaxis against mycobacterium avium-intracellulare?
A 58-year-old woman with HIV infection is brought to the emergency department because of a 2-week history of headaches, blurred vision, and confusion. Her current medications include antiretroviral therapy and trimethoprim-sulfamethoxazole. Neurological examination shows ataxia and memory impairment. Her CD4+ T-lymphocyte count is 90/μL. Cerebrospinal fluid analysis shows lymphocytic predominant pleocytosis, and PCR is positive for Epstein-Barr virus DNA. An MRI of the brain with contrast shows a solitary, weakly ring-enhancing lesion with well-defined borders involving the corpus callosum. Which of the following is the most likely diagnosis?
A 44-year-old man is brought to the emergency department by his daughter for a 1-week history of right leg weakness, unsteady gait, and multiple falls. During the past 6 months, he has become more forgetful and has sometimes lost his way along familiar routes. He has been having difficulties operating simple kitchen appliances such as the dishwasher and the coffee maker. He has recently become increasingly paranoid, agitated, and restless. He has HIV, hypertension, and type 2 diabetes mellitus. His last visit to a physician was more than 2 years ago, and he has been noncompliant with his medications. His temperature is 37.2 °C (99.0 °F), blood pressure is 152/68 mm Hg, pulse is 98/min, and respirations are 14/min. He is somnolent and slightly confused. He is oriented to person, but not place or time. There is mild lymphadenopathy in the cervical, axillary, and inguinal areas. Neurological examination shows right lower extremity weakness with normal tone and no other focal deficits. Laboratory studies show: Hemoglobin 9.2 g/dL Leukocyte count 3600/mm3 Platelet count 140,000/mm3 CD4+ count 56/μL HIV viral load > 100,000 copies/mL Serum Cryptococcal antigen negative Toxoplasma gondii IgG positive An MRI of the brain shows disseminated, nonenhancing white matter lesions with no mass effect. Which of the following is the most likely diagnosis?
A 40-year-old man with AIDS comes to the physician because of a 3-week history of intermittent fever, abdominal pain, and diarrhea. He has also had a nonproductive cough and a 3.6-kg (8-lb) weight loss in this period. He was treated for pneumocystis pneumonia 2 years ago. He has had skin lesions on his chest for 6 months. Five weeks ago, he went on a week-long hiking trip in Oregon. Current medications include efavirenz, tenofovir, and emtricitabine. He says he has had trouble adhering to his medication. His temperature is 38.3°C (100.9°F), pulse is 96/min, and blood pressure is 110/70 mm Hg. Examination shows oral thrush on his palate and a white, non-scrapable plaque on the left side of the tongue. There is axillary and inguinal lymphadenopathy. There are multiple violaceous plaques on the chest. Crackles are heard on auscultation of the chest. Abdominal examination shows mild, diffuse tenderness throughout the lower quadrants. The liver is palpated 2 to 3 cm below the right costal margin, and the spleen is palpated 1 to 2 cm below the left costal margin. Laboratory studies show: Hemoglobin 12.2 g/dL Leukocyte count 4,800/mm3 CD4+ T-lymphocytes 44/mm3 (Normal ≥ 500 mm3) Platelet count 258,000/mm3 Serum Na+ 137 mEq/L Cl- 102 mEq/L K+ 4.9 mEq/L Alkaline phosphatase 202 U/L One set of blood culture grows acid-fast organisms. A PPD skin test shows 4 mm of induration. Which of the following is the most appropriate pharmacotherapy for this patient's condition?
A 34-year-old man comes to the physician for a routine health maintenance examination. He was diagnosed with HIV 8 years ago. He is currently receiving triple antiretroviral therapy. He is sexually active and uses condoms consistently. He is planning a trip to Thailand with his partner to celebrate his 35th birthday in 6 weeks. His last tetanus and diphtheria booster was given 4 years ago. He received three vaccinations against hepatitis B 5 years ago. He had chickenpox as a child. Other immunization records are unknown. Vital signs are within normal limits. Cardiopulmonary examination shows no abnormalities. Leukocyte count shows 8,700/mm3, and CD4+ T-lymphocyte count is 480 cells/mm3 (Normal ≥ 500); anti-HBs is 150 mIU/mL. Which of the following recommendations is most appropriate at this time?
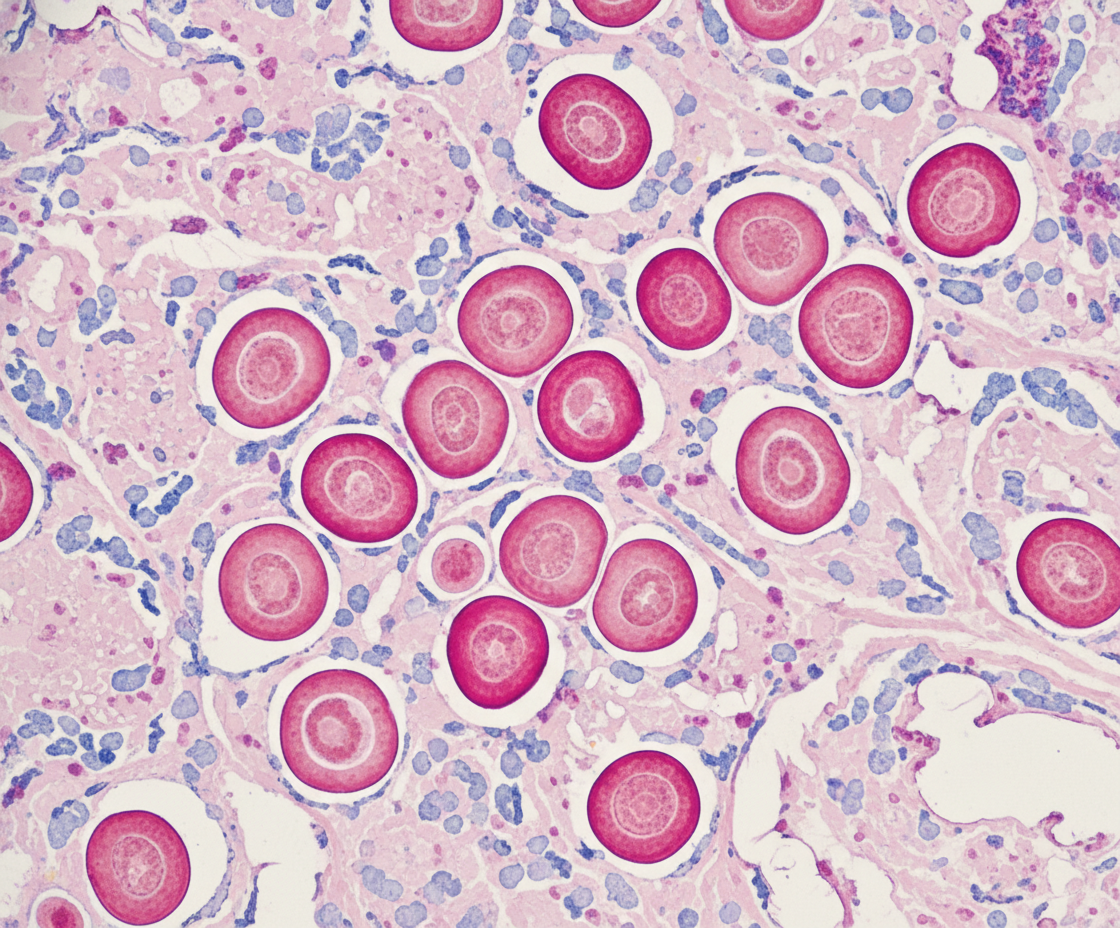
A 37-year-old man comes to the physician because of fever, night sweats, malaise, dyspnea, and a productive cough with bloody sputum for 4 days. He was diagnosed with HIV infection 15 years ago and has not been compliant with his medication regimen. Physical examination shows diminished breath sounds over the left lung fields. An x-ray of the chest shows an ill-defined lesion in the upper lobe of the left lung. A CT-guided biopsy of the lesion is performed; a photomicrograph of the biopsy specimen stained with mucicarmine is shown. Which of the following is the most likely causal organism?
A 33-year-old man with HIV comes to the physician because of a nonproductive cough and shortness of breath for 3 weeks. He feels tired after walking up a flight of stairs and after long conversations on the phone. He appears chronically ill. His temperature is 38.5°C (101.3°F), and pulse is 110/min. Pulse oximetry on room air shows an oxygen saturation of 95%. Upon walking, his oxygen saturation decreases to 85%. Cardiopulmonary examination is normal. Laboratory studies show a CD4+ T-lymphocyte count of 176/mm3 (N > 500). Results of urine Legionella antigen testing are negative. A CT scan of the chest shows diffuse, bilateral ground-glass opacities. Microscopic examination of fluid obtained from bronchoalveolar lavage will most likely show which of the following findings?
An HIV-positive patient with a CD4+ count of 45 is receiving recommended first-line treatment for a case of cytomegalovirus retinitis. Coadministration with which of the following agents would be most likely to precipitate a deficiency of neutrophils in this patient?
A 33-year-old HIV-positive male is seen in clinic for follow-up care. When asked if he has been adhering to his HIV medications, the patient exclaims that he has been depressed, thus causing him to not take his medication for six months. His CD4+ count is now 33 cells/mm3. What medication(s) should he take in addition to his anti-retroviral therapy?
A 57-year-old woman with non-small cell lung cancer comes to the physician 4 weeks after her tumor was resected. She takes no medications. The physician starts her on a treatment regimen that includes vinblastine. This treatment puts the patient at highest risk for which of the following?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app