
Central nervous system infections — MCQs

A 10-year-old boy is brought to the emergency department by his parents because of a dull persistent headache beginning that morning. He has nausea and has vomited twice. During the past four days, the patient has had left-sided ear pain and fever, but his parents did not seek medical attention. He is from Thailand and is visiting his relatives in the United States for the summer. There is no personal or family history of serious illness. He is at the 45th percentile for height and 40th percentile for weight. He appears irritable. His temperature is 38.5°C (101.3°F), pulse is 110/min, and blood pressure is 98/58 mm Hg. The pupils are equal and reactive to light. Lateral gaze of the left eye is limited. The left tympanic membrane is erythematous with purulent discharge. There is no nuchal rigidity. Which of the following is the most appropriate next step in management?
A 15-year-old boy is brought to the Emergency department by ambulance from school. He started the day with some body aches and joint pain but then had several episodes of vomiting and started complaining of a terrible headache. The school nurse called for emergency services. The boy was born at 39 weeks gestation via spontaneous vaginal delivery. He is up to date on all vaccines and is meeting all developmental milestones. Past medical history is noncontributory. He is a good student and enjoys sports. At the hospital, his blood pressure is 120/80 mm Hg, heart rate is 105/min, respiratory rate is 21/min, and his temperature is 38.9°C (102.0°F). On physical exam, he appears drowsy with neck stiffness and sensitivity to light. Kernig’s sign is positive. An ophthalmic exam is performed followed by a lumbar puncture. An aliquot of cerebrospinal fluid is sent to microbiology. A gram stain shows gram-negative diplococci. A smear is prepared on blood agar and grows round, smooth, convex colonies with clearly defined edges. Which of the following would identify the described pathogen?
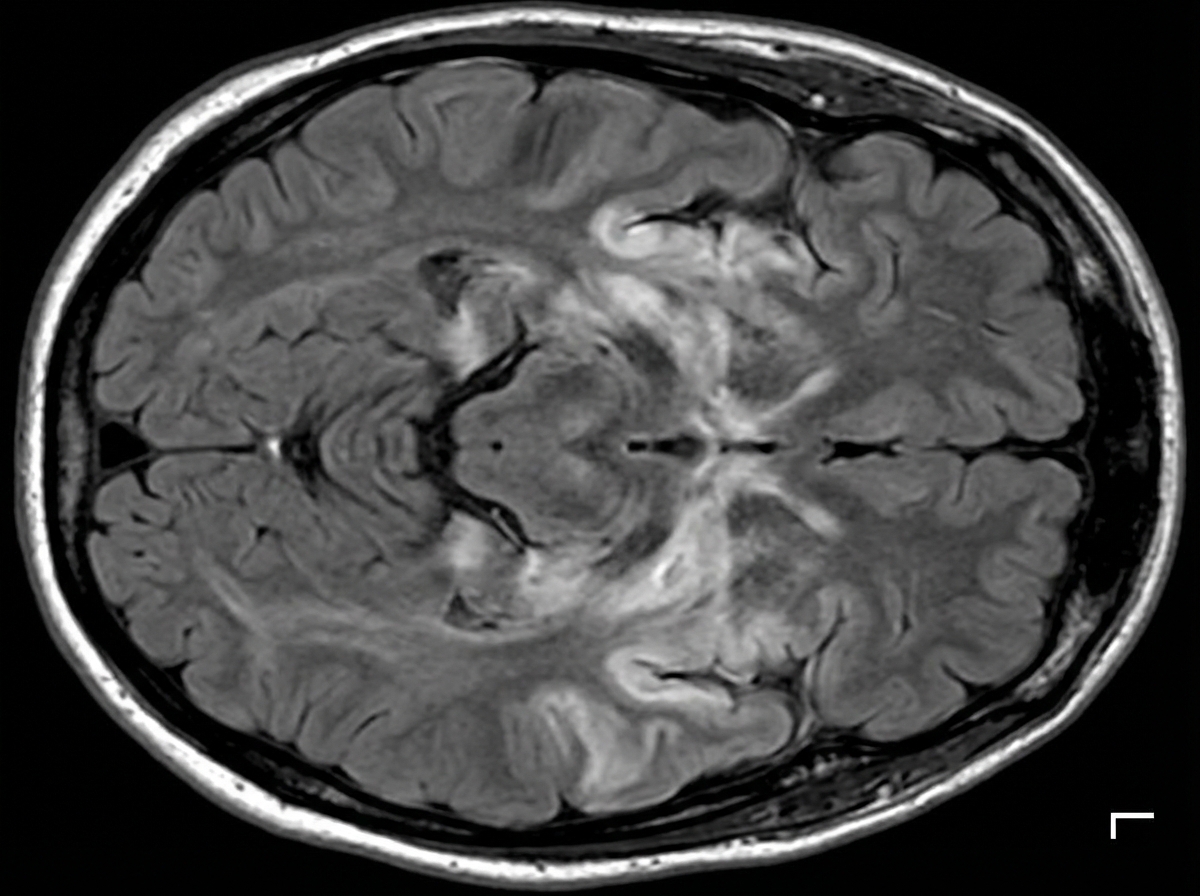
A 27-year-old man is brought to the emergency department by his friends in a confused state. He was doing fine 5 days ago when he started to complain of fever and flu-like symptoms. His fever was low-grade and associated with a headache. For the past 2 days, he has become increasingly irritable, confused, and was getting angry at trivial things. Past medical history is unremarkable. He is a college student and is physically active. He smokes cigarettes occasionally. He drinks alcohol socially. He is sexually active with his girlfriend and they use condoms inconsistently. Physical examination reveals: blood pressure 120/80 mm Hg, heart rate 108/min, respiratory rate 10/min, and temperature 37.4°C (99.4°F). He is confused and disoriented. Pupils are 3 mm in diameter and respond to light sluggishly. He is moving all his limbs spontaneously. His neck is supple. MRI of the brain is shown in the picture. Cerebrospinal fluid (CSF) reveals an opening pressure of 16 cm of H20, a total leukocyte count of 112/mm3 with 85% lymphocytes, the protein of 42 mg/dL, and glucose of 58 mg/dL. What is the best treatment for this condition?
A 26-year-old female with AIDS (CD4 count: 47) presents to the emergency department in severe pain. She states that over the past week she has been fatigued and has had a progressively worse headache and fever. These symptoms have failed to remit leading her to seek care in the ED. A lumbar puncture is performed which demonstrates an opening pressure of 285 mm H2O, increased lymphocytes, elevated protein, and decreased glucose. The emergency physician subsequently initiates treatment with IV amphotericin B and PO flucytosine. What additional treatment in the acute setting may be warranted in this patient?
A 34-year-old woman presents with confusion, drowsiness, and headache. The patient’s husband says her symptoms began 2 days ago and have progressively worsened with an acute deterioration of her mental status 2 hours ago. The patient describes the headaches as severe, localized to the frontal and periorbital regions, and worse in the morning. Review of symptoms is significant for a mild, low-grade fever, fatigue, and nausea for the past week. Past medical history is significant for HIV infection for which she is not currently receiving therapy. Her CD4+ T cell count last month was 250/mm3. The blood pressure is 140/85 mm Hg, the pulse rate is 90/min, and the temperature is 37.7°C (100.0°F). On physical examination, the patient is conscious but drowsy. Papilledema is present. No pain is elicited with extension of the leg at the knee joint. The remainder of the physical examination is negative. Laboratory findings, including panculture, are ordered. A noncontrast CT scan of the head is negative and is followed by a lumbar puncture. CSF analysis is significant for: Opening pressure 250 mm H2O (70-180 mm H2O) Glucose 30 mg/dL (40-70 mg/dL) Protein 100 mg/dL (<40 mg/dL) Cell count 20/mm3 (0-5/mm3) Which of the following additional findings would most likely be found in this patient?
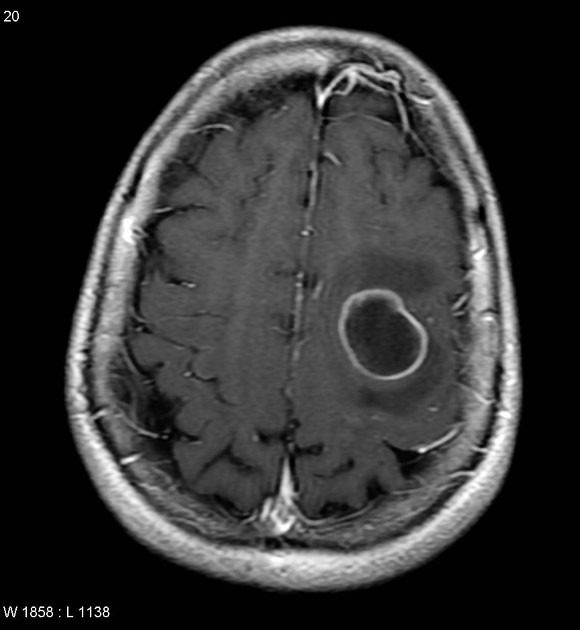
A 42-year-old man is brought to the physician 25 minutes after an episode of violent jerky movements of his hands and legs that lasted for 5 minutes. After the episode, he had difficulty conversing. For the past 10 days, he has had a left-sided headache and nausea. Apart from a history of recurrent ear infections treated with antibiotics, he reports no other personal or family history of serious illness. He works as an assistant at a veterinarian clinic. He appears ill and is oriented to place and person only. His temperature is 37.8°C (100°F), pulse is 102/min, and blood pressure 112/78 mm Hg. Examination shows bilateral optic disc swelling. There is no lymphadenopathy. Muscle strength and tone is normal in all extremities. Deep tendon reflexes are 2+ bilaterally. Plantar reflex shows a flexor response bilaterally. Laboratory studies show a CD4 count within the reference range. An MRI of the brain is shown. Intravenous mannitol and levetiracetam are administered. Which of the following is the most appropriate next step in management?
A 21-year-old G3P2 woman presents to her obstetrician at 6 weeks gestation for routine prenatal care. Her past medical history includes obesity and gestational diabetes. She has had two spontaneous vaginal deliveries at term. One infant was macrosomic with hypoglycemia, but otherwise, she has had no complications. Her physician informs her that she must start taking a multivitamin with folic acid daily. The defect that folic acid supplementation protects against arises in tissue that is derived from which germ cell layer?
A 32-year-old woman presents with a 3-month history of intermittent blurred vision and problems walking. The patient states that she often feels “pins and needles” in her legs that cause her problems when she’s walking. The patient is afebrile, and her vital signs are within normal limits. An autoimmune disorder is suspected. Which of the following findings would most likely be present in this patient?
A 3-year-old boy is brought to the physician for the evaluation of recurrent skin lesions. The episodes of lesions started at the age of 3 months. He has also had several episodes of respiratory tract infections, enlarged lymph nodes, and recurrent fevers since birth. The boy attends daycare. The patient's immunizations are up-to-date. He is at the 5th percentile for length and 10th percentile for weight. He appears ill. Temperature is 38°C (100.4°F). Examination shows several raised, erythematous lesions of different sizes over the face, neck, groin, and extremities; some are purulent. Bilateral cervical and axillary lymphadenopathy are present. What is the most likely underlying mechanism of this patient's symptoms?
A 33-year-old man is brought to the emergency department 20 minutes after he fell from the roof of his house. On arrival, he is unresponsive to verbal and painful stimuli. His pulse is 72/min and blood pressure is 132/86 mm Hg. A CT scan of the head shows a fracture in the anterior cranial fossa and a 1-cm laceration in the left anterior orbital gyrus. If the patient survives, which of the following would ultimately be the most common cell type at the injured region of the frontal lobe?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app