
Infectious diseases (sepsis, endocarditis) — MCQs

On this page
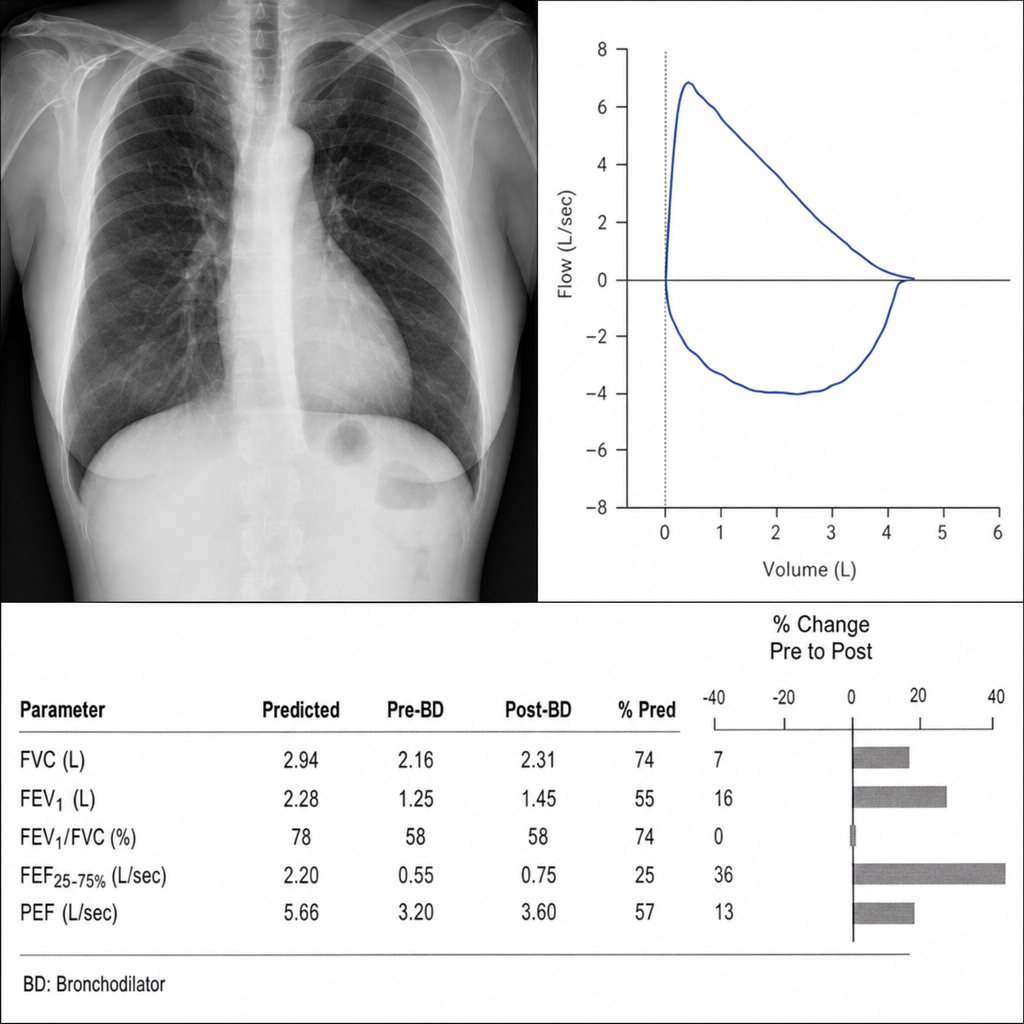
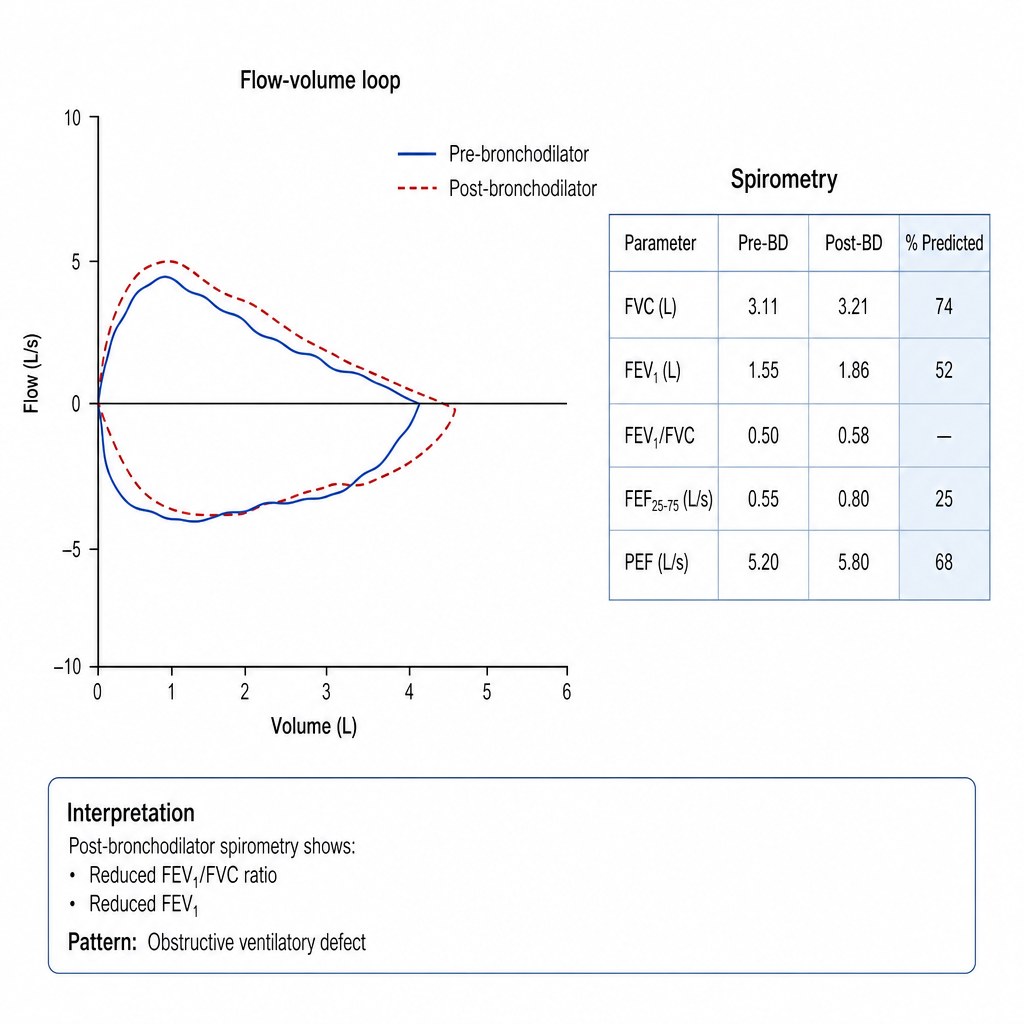
A 54-year-old woman with a 30 pack-year smoking history presents with progressive dyspnea over 6 months, a chronic productive cough, and two respiratory hospitalizations in the past year. She denies orthopnea or paroxysmal nocturnal dyspnea. Examination reveals a barrel-shaped chest, prolonged expiration with diffuse expiratory wheezes, and mild lower extremity edema. Chest X-ray shows hyperinflation with flattened diaphragms. Spirometry is performed and reveals an FEV₁/FVC ratio of 0.58 (post-bronchodilator), an FEV₁ of 52% predicted, and a flow-volume loop with a characteristic concave (scooped) expiratory limb consistent with dynamic airway collapse. Which of the following best describes the spirometric pattern and its implication for management?
A 29-year-old woman presents with 4 months of fatigue, pallor, and exertional dyspnea. She has no significant past medical history and takes no medications. She reports heavy menstrual periods since adolescence. Vital signs are normal. Laboratory results: hemoglobin 7.2 g/dL, MCV 68 fL, RDW 19%, reticulocyte count 1.1%, serum ferritin 6 ng/mL, TIBC 480 μg/dL, serum iron 28 μg/dL. She is started on oral ferrous sulfate 325 mg three times daily. Six weeks later, her hemoglobin is 8.1 g/dL. Which of the following is the most appropriate next step?

A 55-year-old man with a 40-pack-year smoking history presents with progressive dyspnea on exertion and a chronic productive cough. Pulmonary function testing is performed. His post-bronchodilator FEV1/FVC ratio is 0.58, and his FEV1 is 52% of predicted. He has had two exacerbations requiring oral steroids in the past year but no hospitalizations. His current regimen includes a short-acting beta-agonist as needed. Which of the following is the most appropriate modification to his maintenance therapy?
A 42-year-old IV drug user with known HIV (CD4 count 85 cells/mm³, not on antiretroviral therapy) presents with fever and a new heart murmur. Blood cultures grow Candida albicans. Transesophageal echocardiogram shows a 20 mm vegetation on the tricuspid valve with moderate regurgitation but no heart failure. He is treated with micafungin and shows clinical improvement after 1 week. Evaluate the definitive management strategy for this patient.
A 72-year-old man with severe sepsis from pneumonia is started on norepinephrine and broad-spectrum antibiotics. After 12 hours, his blood pressure is 90/55 mmHg on norepinephrine 0.4 mcg/kg/min, heart rate 95/min, and lactate has decreased from 4.5 to 2.8 mmol/L. Random cortisol level is 18 mcg/dL. He has a history of COPD on chronic prednisone 10 mg daily. Evaluate the role of corticosteroid therapy in this patient.
Practice by Chapter
Sepsis and septic shock
Practice Questions
Infective endocarditis
Practice Questions
Pneumonia (community-acquired, hospital-acquired)
Practice Questions
Urinary tract infections
Practice Questions
Skin and soft tissue infections
Practice Questions
Central nervous system infections
Practice Questions
Intra-abdominal infections
Practice Questions
Sexually transmitted infections
Practice Questions
HIV/AIDS
Practice Questions
Tuberculosis
Practice Questions
Opportunistic infections
Practice Questions
Fever of unknown origin
Practice Questions
Antimicrobial stewardship
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app