
Ulcerative colitis pathophysiology — MCQs

A 24-year-old woman comes to the physician because of progressively worsening episodes of severe, crampy abdominal pain and nonbloody diarrhea for the past 3 years. Examination of the abdomen shows mild distension and generalized tenderness. There is a fistula draining stool in the perianal region. Immunohistochemistry shows dysfunction of the nucleotide oligomerization binding domain 2 (NOD2) protein. This dysfunction most likely causes overactivity of which of the following immunological proteins in this patient?
A 24-year-old woman presents to the clinic with chronic abdominal discomfort and cramping. She seeks medical attention now as she is concerned about the diarrhea that she has developed that is occasionally mixed with tiny streaks of blood. Her medical history is significant for lactose intolerance and asthma. She has a family history of wheat allergy and reports that she has tried to make herself vomit on several occasions to lose weight. After counseling the patient about the dangers of bulimia, physical examination reveals the rectum is red, inflamed, tender, and a perirectal abscess is seen draining purulent material. Colonoscopy demonstrates scattered mucosal lesions involving the colon and terminal ileum. A complete blood count is given below: Hb%: 10 gm/dL Total count (WBC): 12,500/mm3 Differential count: Neutrophils: 50% Lymphocytes: 40% Monocytes: 5% ESR: 22 mm/hr What is the most likely diagnosis?
A 22-year-old woman presents to the emergency department with a 3-day history of fever and abdominal pain. She says that the pain is located in the left lower quadrant of the abdomen and feels crampy in nature. The pain has been associated with bloody diarrhea and joint tenderness. She has no past medical history but says that she returned 2 weeks ago from vacation in Asia where she tried many new foods. Her family history is significant for multiple cancers in close relatives. Physical exam reveals swollen ulcers on her legs, and colonoscopy reveals contiguous ulcerations from the rectum through the descending colon. Which of the following is associated with the most likely cause of this patient's symptoms?
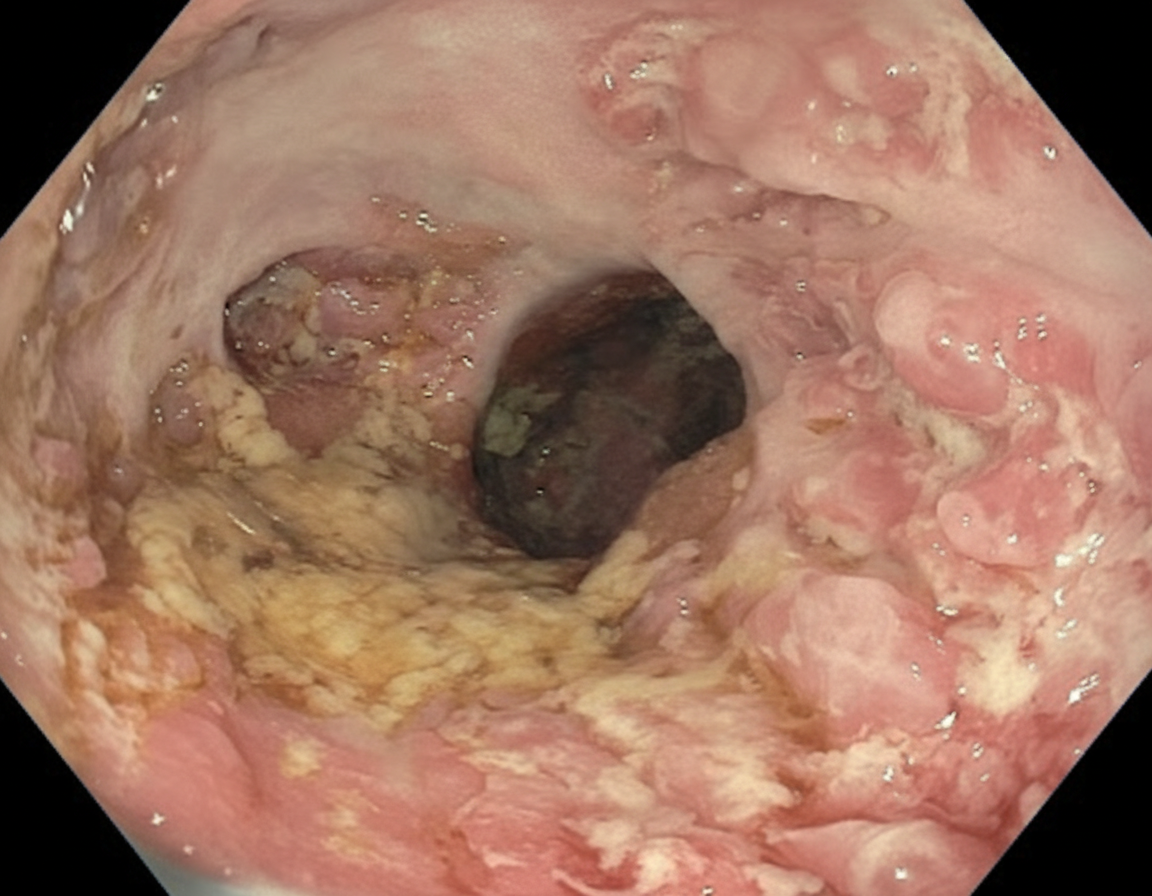
A 28-year-old man comes to the physician because of a 6-month history of progressive fatigue and intermittent diarrhea. During this time, he has had a 6-kg (13-lb) weight loss. Physical examination shows pale conjunctivae. Abdominal examination shows tenderness to palpation in the lower quadrants. An image from a colonoscopy of the descending colon is shown. Further evaluation is most likely to show which of the following findings?
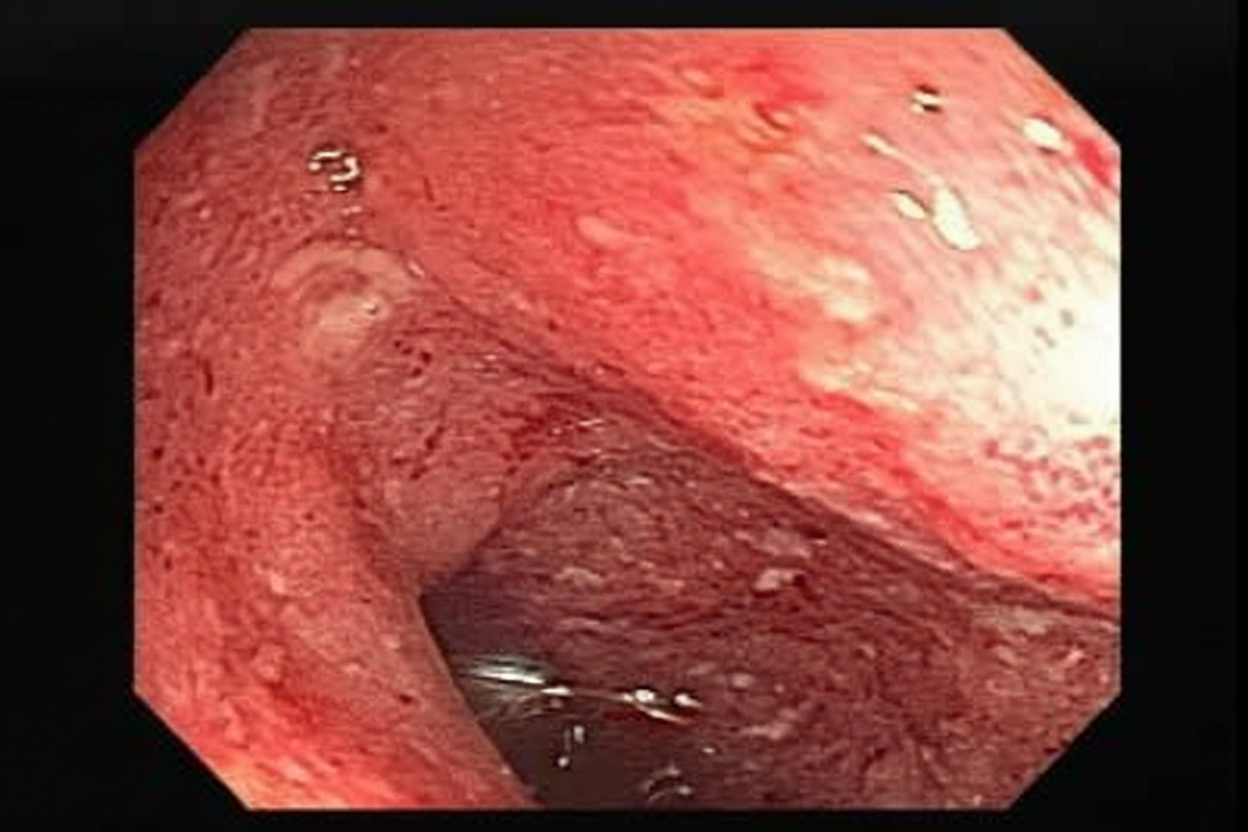
A 23-year-old female presents with a seven-day history of abdominal pain, and now bloody diarrhea that brings her to her primary care physician. Review of systems is notable for a 12-pound unintentional weight loss and intermittent loose stools. She has a family history notable for a father with CAD and a mother with primary sclerosing cholangitis. Upon further workup, she is found to have the following on colonoscopy and biopsy, Figures A and B respectively. Serum perinuclear antineutrophil cytoplasmic antibodies (P-ANCA) is positive. This patient's disease is likely to also include which of the following features?
A 42-year-old man comes to the physician because of a 6-week history of intermittent fever, abdominal pain, bloody diarrhea, and sensation of incomplete rectal emptying. He also has had a 4.5-kg (10-lb) weight loss over the past 3 months. Abdominal examination shows diffuse tenderness. Colonoscopy shows circumferential erythematous lesions that extend without interruption from the anal verge to the cecum. A biopsy specimen taken from the rectum shows mucosal and submucosal inflammation with crypt abscesses. This patient is most likely at risk of developing colon cancer with which of the following characteristics?
A 34-year-old woman with no significant prior medical history presents to the clinic with several days of bloody stool. She also complains of constipation and straining, but she has no other symptoms. She has no family history of colorectal cancer or inflammatory bowel disease. She does not smoke or drink alcohol. Her vital signs are as follows: blood pressure is 121/81 mm Hg, heart rate is 77/min, and respiratory rate is 15/min. There is no abdominal discomfort on physical exam, and a digital rectal exam reveals bright red blood. Of the following, which is the most likely diagnosis?
A 32-year-old man comes to the physician for a follow-up examination. He has a 2-month history of increasing generalized fatigue and severe pruritus. He has hypertension and ulcerative colitis which was diagnosed via colonoscopy 5 years ago. Current medications include lisinopril and rectal mesalamine. He is sexually active with 2 female partners and uses condoms inconsistently. His temperature is 37.3°C (99.1°F), pulse is 86/min, and blood pressure is 130/84 mm Hg. Examination shows scleral icterus and multiple scratch marks on the trunk and extremities. The lungs are clear to auscultation. The abdomen is soft and nontender. The remainder of the examination shows no abnormalities. Laboratory studies show: Hemoglobin 11.5 g/dL Leukocyte count 7500/mm3 Platelet count 280,000/mm3 Serum Na+ 138 mEq/L Cl- 101 mEq/L K+ 4.7 mEq/L Urea nitrogen 18 mg/dL Glucose 91 mg/dL Creatinine 0.8 mg/dL Bilirubin Total 1.5 mg/dL Direct 0.9 mg/dL Alkaline phosphatase 460 U/L AST 75 U/L ALT 78 U/L Anti-nuclear antibody negative Antimitochondrial antibodies negative Abdominal ultrasound shows thickening of the bile ducts and focal bile duct dilatation. Which of the following is the most likely diagnosis?
A 31-year-old woman comes to the emergency department because of a 4-day history of fever and diarrhea. She has abdominal cramps and frequent bowel movements of small quantities of stool with blood and mucus. She has had multiple similar episodes over the past 8 months. Her temperature is 38.1°C (100.6°F), pulse is 75/min, and blood pressure is 130/80 mm Hg. Bowel sounds are normal. The abdomen is soft. There is tenderness to palpation in the left lower quadrant with guarding and no rebound. She receives appropriate treatment and recovers. Two weeks later, colonoscopy shows polypoid growths flanked by linear ulcers. A colonic biopsy specimen shows mucosal edema with distorted crypts and inflammatory cells in the lamina propria. Which of the following is the most appropriate recommendation for this patient?
A 22-year-old man presents to the emergency department with abdominal pain. The patient states that he has had right lower quadrant abdominal pain for "a while now". The pain comes and goes, and today it is particularly painful. The patient is a college student studying philosophy. He drinks alcohol occasionally and is currently sexually active. He states that sometimes he feels anxious about school. The patient's father died of colon cancer at the age of 55, and his mother died of breast cancer when she was 57. The patient has a past medical history of anxiety and depression which is not currently treated. Review of systems is positive for bloody diarrhea. His temperature is 99.5°F (37.5°C), blood pressure is 100/58 mmHg, pulse is 120/min, respirations are 17/min, and oxygen saturation is 98% on room air. Cardiopulmonary exam is within normal limits. Abdominal exam reveals diffuse tenderness. A fecal occult blood test is positive. Which of the following is the most likely diagnosis?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app