
IBD — MCQs

On this page
A 28-year-old woman presents to the clinic with complaints of occasional low-grade fever and joint pain for 1 month. She also complains of morning stiffness in the proximal interphalangeal joints of both hands, which lasts for 5 to 10 minutes. She recently noticed a pink rash on her nose and cheekbones. Her family history is significant for similar complaints in her mother. She is not taking any medications. On examination, her temperature is 37.6°C (99.6°F), pulse is 74/min, blood pressure is 110/70 mm Hg, and respirations are 18/min. Aphthous ulcers are noted on her oral mucosa. Which of the following tests would be most specific for confirming the diagnosis in this patient?
A 35-year-old woman comes to the physician because of a 3-month history of worsening fatigue. She has difficulty concentrating at work despite sleeping well most nights. Three years ago, she was diagnosed with Crohn disease. She has about 7 non-bloody, mildly painful bowel movements daily. Her current medications include 5-aminosalicylic acid and topical budesonide. She does not smoke or drink alcohol. She appears pale. Her temperature is 37.9°C (100.2°F), pulse is 92/min, and blood pressure is 110/65 mmHg. The abdomen is diffusely tender to palpation, with no guarding. Laboratory results show: Hemoglobin 10.5 g/dL Mean corpuscular volume 83 μm3 Reticulocytes 0.2 % Platelets 189,000/mm3 Serum Iron 21 μg/dL Total iron binding capacity 176 μg/dL (N=240–450) A blood smear shows anisocytosis. Which of the following is the most appropriate next step in treatment?
A 36-year-old man comes to the emergency department for the evaluation of recurrent bloody diarrhea for 4 weeks. During this time, he has also had intermittent abdominal pain. His symptoms have worsened over the past 2 days and he has also had fever and several episodes of nonbloody vomiting. He was diagnosed with ulcerative colitis three years ago but has had difficulty complying with his drug regimen. His temperature is 38.8°C (100.9°F), pulse is 112/min and regular, and blood pressure is 90/50 mm Hg. Abdominal examination shows a distended abdomen with no guarding or rebound; bowel sounds are hypoactive. Hemoglobin concentration is 10.1 g/dL, leukocyte count is 15,000/mm3, and erythrocyte sedimentation rate is 50 mm/h. Fluid resuscitation is initiated. In addition to complete bowel rest, which of the following is the most appropriate next step in the management of this patient?
A 29-year-old man presents to clinic with a complaint of fatigue that has developed over the past 6 months. Upon questioning, he endorses abdominal pain, non-bloody diarrhea, and decreased appetite over the past year. He denies recent travel outside of the country or eating uncooked meats. On exam, his temperature is 99.0°F (37.2°C), blood pressure is 126/78 mmHg, pulse is 93/min, and respirations are 12/min. Notably, the abdominal exam is unremarkable aside from some tenderness to palpation near the umbilicus. His colonoscopy demonstrates perianal inflammation with a normal rectum, and biopsies of suspicious lesions in the transverse colon reveal transmural inflammation. Which one of the following is most strongly associated with the patient’s condition?
A 33-year-old woman presents to the clinic complaining of yellowish discoloration of her skin and eyes, mild fever, and body aches. She has had this problem for 6 months, but it has become worse over the past few weeks. She also complains of repeated bouts of bloody diarrhea and abdominal pain. The past medical history is noncontributory. She takes no medication. Both of her parents are alive with no significant disease. She works as a dental hygienist and drinks wine occasionally on weekends. Today, the vital signs include blood pressure 110/60 mm Hg, pulse rate 90/min, respiratory rate 19/min, and temperature 36.6°C (97.8°F). On physical examination, she appears uncomfortable. The skin and sclera are jaundiced. The heart has a regular rate and rhythm, and the lungs are clear to auscultation bilaterally. The abdomen is soft with mild hepatosplenomegaly. There is no tenderness or rebound tenderness. The digital rectal examination reveals blood and mucus in the rectal vault. Laboratory studies show: Serum sodium 140 mEq/L Serum potassium 3.8 mEq/L Alanine aminotransferase (ALT) 250 U/L Aspartate aminotransferase (AST) 170 U/L Alkaline phosphatase (ALP) 120 U/L Which of the following antibodies would you expect to find in this patient?
A 27-year-old female has a history of periodic bloody diarrhea over several years. Colonoscopy shows sigmoid colon inflammation, and the patient complains of joint pain in her knees and ankles. You suspect inflammatory bowel disease. Which of the following would suggest a diagnosis of Crohn disease:
An 18-year-old man presents with bloody diarrhea and weight loss. He undergoes endoscopic biopsy which shows pseudopolyps. Biopsies taken during the endoscopy show inflammation only involving the mucosa and submucosa. He is diagnosed with an inflammatory bowel disease. Which of the following characteristics was most likely present?
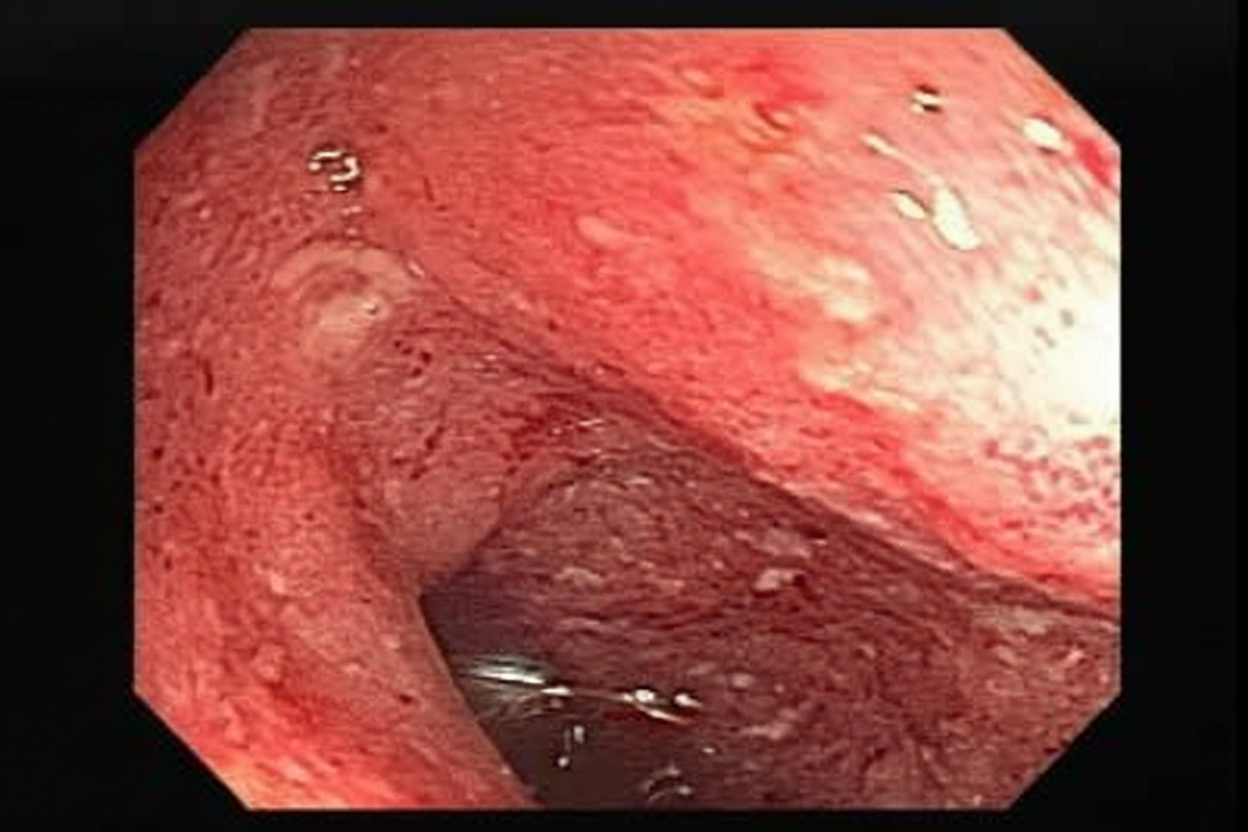
A 23-year-old female presents with a seven-day history of abdominal pain, and now bloody diarrhea that brings her to her primary care physician. Review of systems is notable for a 12-pound unintentional weight loss and intermittent loose stools. She has a family history notable for a father with CAD and a mother with primary sclerosing cholangitis. Upon further workup, she is found to have the following on colonoscopy, Figure A. Serum perinuclear antineutrophil cytoplasmic antibodies (P-ANCA) is positive. This patient's disease is likely to also include which of the following features?
A 27-year-old male presents to his primary care physician complaining of pain with urination and eye redness. He reports that he developed these symptoms approximately one week ago. He also has noticed left knee and right heel pain that started a few days ago. He denies any recent trauma. He had an episode of abdominal pain and diarrhea ten days ago that resolved. He has otherwise felt well. On exam, he walks with a limp and his conjunctivae are erythematous. Laboratory findings are notable for an elevated erythrocyte sedimentation rate (ESR) and elevated C-reactive protein (CRP). Which of the following is most likely associated with this patient’s condition?
A 34-year-old man presents to his dermatologist with white scaly papules and plaques on his extensor arms, elbows, knees, and shins. Scaly and flaky eruptions are also present on his ears, eyebrows, and scalp. He describes the lesions as being itchy and irritating. When the scales are scraped away, pinpoint bleeding is noted. His vital signs are unremarkable, and physical examination is otherwise within normal limits. Which of the following is the best initial test for this patient’s condition?
Practice by Chapter
Crohn's disease pathophysiology
Practice Questions
Ulcerative colitis pathophysiology
Practice Questions
Diagnostic approach to IBD
Practice Questions
Extraintestinal manifestations
Practice Questions
Medical management of Crohn's disease
Practice Questions
Medical management of ulcerative colitis
Practice Questions
Biologic therapies for IBD
Practice Questions
Surgical management in IBD
Practice Questions
Nutritional considerations in IBD
Practice Questions
IBD in pregnancy
Practice Questions
Cancer risk and surveillance in IBD
Practice Questions
IBD-related complications
Practice Questions
IBD in special populations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app