
IBD-related complications — MCQs

A 23-year-old man complains of lower back pain that began approximately 6 months ago. He is unsure why he is experiencing this pain and notices that this pain is worse in the morning after waking up and improves with physical activity. Ibuprofen provides significant relief. He denies bowel and bladder incontinence or erectile dysfunction. Physical exam is notable for decreased chest expansion, decreased spinal range of motion, 5/5 strength in both lower extremities, 2+ patellar reflexes bilaterally, and an absence of saddle anesthesia. Which of the following is the most appropriate next test for this patient?
A 32-year-old man comes to the physician for a follow-up examination. He has a 2-month history of increasing generalized fatigue and severe pruritus. He has hypertension and ulcerative colitis which was diagnosed via colonoscopy 5 years ago. Current medications include lisinopril and rectal mesalamine. He is sexually active with 2 female partners and uses condoms inconsistently. His temperature is 37.3°C (99.1°F), pulse is 86/min, and blood pressure is 130/84 mm Hg. Examination shows scleral icterus and multiple scratch marks on the trunk and extremities. The lungs are clear to auscultation. The abdomen is soft and nontender. The remainder of the examination shows no abnormalities. Laboratory studies show: Hemoglobin 11.5 g/dL Leukocyte count 7500/mm3 Platelet count 280,000/mm3 Serum Na+ 138 mEq/L Cl- 101 mEq/L K+ 4.7 mEq/L Urea nitrogen 18 mg/dL Glucose 91 mg/dL Creatinine 0.8 mg/dL Bilirubin Total 1.5 mg/dL Direct 0.9 mg/dL Alkaline phosphatase 460 U/L AST 75 U/L ALT 78 U/L Anti-nuclear antibody negative Antimitochondrial antibodies negative Abdominal ultrasound shows thickening of the bile ducts and focal bile duct dilatation. Which of the following is the most likely diagnosis?
A 32-year-old man comes to the emergency department because of recurrent episodes of vomiting for 1 day. He has had over 15 episodes of bilious vomiting. During this period he has had cramping abdominal pain but has not had a bowel movement or passed flatus. He does not have fever or diarrhea. He was diagnosed with Crohn disease at the age of 28 years which has been well controlled with oral mesalamine. He underwent a partial small bowel resection for midgut volvulus at birth. His other medications include vitamin B12, folic acid, loperamide, ferrous sulfate, and vitamin D3. He appears uncomfortable and his lips are parched. His temperature is 37.1°C (99.3°F), pulse is 103/min, and blood pressure is 104/70 mm Hg. The abdomen is distended, tympanitic, and tender to palpation over the periumbilical area and the right lower quadrant. Rectal examination is unremarkable. A CT scan of the abdomen shows multiple dilated loops of small bowel with a transition zone in the mid to distal ileum. After 24 hours of conservative management with IV fluid resuscitation, nasogastric bowel decompression, promethazine, and analgesia, his condition does not improve and a laparotomy is scheduled. During the laparotomy, two discrete strictures are noted in the mid-ileum, around 20 cm apart. Which of the following is the most appropriate next step in management?
A 22-year-old woman presents to the emergency department with a 3-day history of fever and abdominal pain. She says that the pain is located in the left lower quadrant of the abdomen and feels crampy in nature. The pain has been associated with bloody diarrhea and joint tenderness. She has no past medical history but says that she returned 2 weeks ago from vacation in Asia where she tried many new foods. Her family history is significant for multiple cancers in close relatives. Physical exam reveals swollen ulcers on her legs, and colonoscopy reveals contiguous ulcerations from the rectum through the descending colon. Which of the following is associated with the most likely cause of this patient's symptoms?
A 37-year-old man presents to his gastroenterologist due to a transaminitis found by his primary care physician (PCP). He reports currently feeling well and has no acute concerns. Medical history is significant for ulcerative colitis treated with 5-aminosalicylate. He recently went on a trip to Mexico and experienced an episode of mild diarrhea. The patient is 5 ft 4 in and weighs 220 lbs (99.8 kg). His temperature is 98°F (36.7°C), blood pressure is 138/88 mmHg, pulse is 90/min, and respirations are 18/min. Physical examination is unremarkable. Laboratory testing demonstrates: Leukocyte count: 7,200 /mm^3 Alkaline phosphatase: 205 U/L Aspartate aminotransferase (AST): 120 U/L Alanine aminotransferase (ALT): 115 U/L Perinuclear antineutrophil cytoplasmic antibody (pANCA): Positive Antimitochondrial antibody: Negative Which of the following is most likely the diagnosis?
A 23-year-old female presents with a seven-day history of abdominal pain, and now bloody diarrhea that brings her to her primary care physician. Review of systems is notable for a 12-pound unintentional weight loss and intermittent loose stools. She has a family history notable for a father with CAD and a mother with primary sclerosing cholangitis. Upon further workup, she is found to have the following on colonoscopy and biopsy, Figures A and B respectively. Serum perinuclear antineutrophil cytoplasmic antibodies (P-ANCA) is positive. This patient's disease is likely to also include which of the following features?
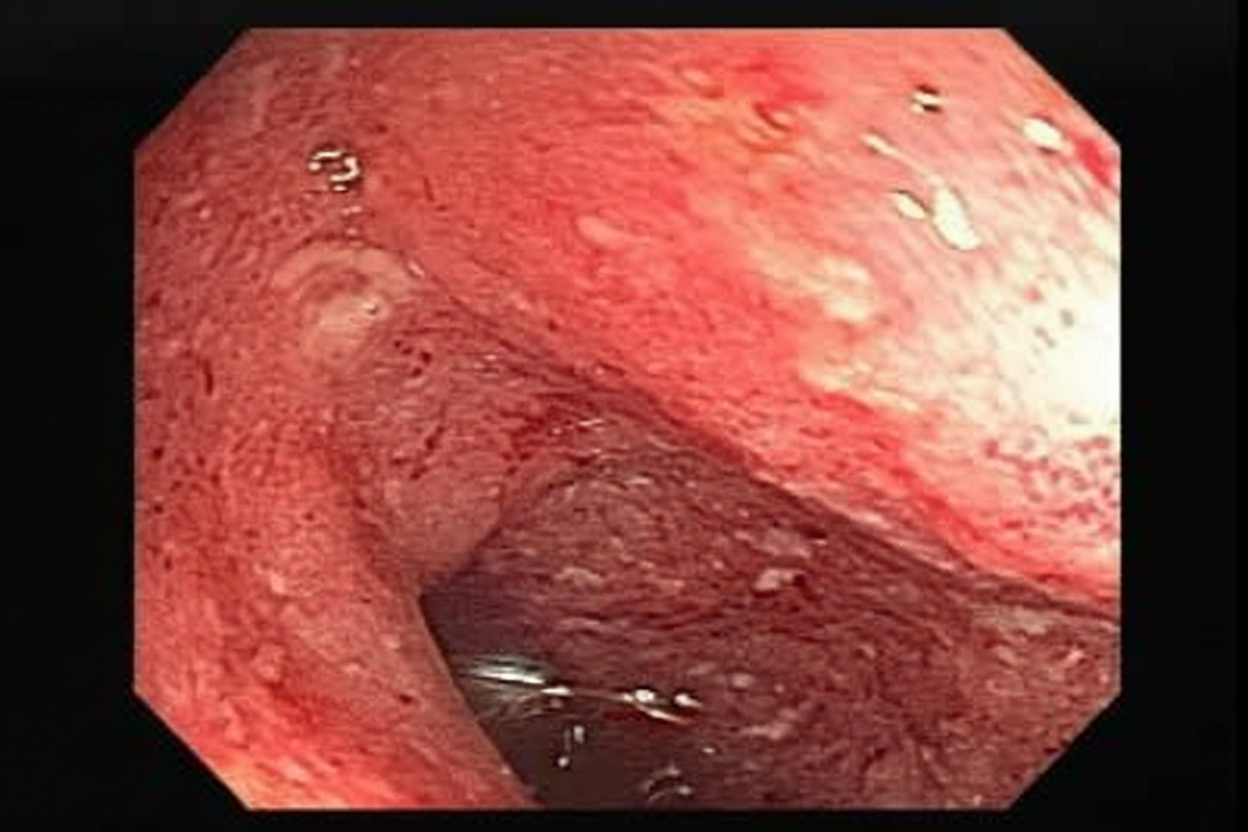
A 22-year-old Caucasian female presents with severe right lower quadrant pain, malaise, and diarrhea. The physician performs an endoscopy and finds disease involvement in the terminal ileum, noting that the disease process is patchy with normal intervening mucosa. The entire wall of the region is thickened and inflamed, which may directly lead to formation of:
A 32-year-old woman presents to her family physician with a long history of depression, irritability, and, more recently, personality changes. As her partner comments, she has stopped engaging in activities she used to enjoy like dancing, drumming lessons, and yoga. The patient denies changes in skin pigmentation and assures she keeps a balanced diet low in fat and carbohydrates. During the physical examination, jaundice and dark rings encircling the iris of the eye are noted, as well as hepatomegaly and gait disturbances. For a follow-up visit, the patient brings a battery of laboratory tests that includes a complete blood count showing normocytic normochromic anemia, a negative Coombs, normal iron levels, normal fasting glucose levels, elevated aminotransferases from the liver biochemical tests, bilirubin, and decreased serum ceruloplasmin levels. Antinuclear antibodies are negative. What is the most likely diagnosis?
A 72-year-old female presents to the emergency department complaining of severe abdominal pain and several days of bloody diarrhea. Her symptoms began with intermittent bloody diarrhea five days ago and have worsened steadily. For the last 24 hours, she has complained of fevers, chills, and abdominal pain. She has a history of ulcerative colitis, idiopathic hypertension, and hypothyroidism. Her medications include hydrochlorothiazide, levothyroxine, and sulfasalazine. In the ED, her temperature is 39.1°C (102.4°F), pulse is 120/min, blood pressure is 90/60 mmHg, and respirations are 20/min. On exam, the patient is alert and oriented to person and place, but does not know the day. Her mucus membranes are dry. Heart and lung exam are not revealing. Her abdomen is distended with marked rebound tenderness. Bowel sounds are hyperactive. Serum: Na+: 142 mEq/L Cl-: 107 mEq/L K+: 3.3 mEq/L HCO3-: 20 mEq/L BUN: 15 mg/dL Glucose: 92 mg/dL Creatinine: 1.2 mg/dL Calcium: 10.1 mg/dL Hemoglobin: 11.2 g/dL Hematocrit: 30% Leukocyte count: 14,600/mm^3 with normal differential Platelet count: 405,000/mm^3 What is the next best step in management?
A 53 year-old woman with history of ulcerative colitis presents to the emergency department with a severe flare. The patient reports numerous bloody loose stools, and has been febrile for two days. Vital signs are: T 101.9 HR 98 BP 121/86 RR 17 Sat 100%. Abdominal exam is notable for markedly distended abdomen with tympani and tenderness to palpation without guarding or rebound. KUB is shown in figure A. CT scan shows markedly dilated descending and sigmoid colon with no perforations. What is the next best step in management for this patient?

Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app