
IBD — MCQs

On this page
A 17-year-old girl is brought to the physician by her parents for the evaluation of belly pain and a pruritic skin rash on her shoulders for the last 6 months. She describes feeling bloated after meals. Over the past 3 months, she has had multiple loose bowel movements per day. She appears thin. She is at the 20th percentile for height and 8th percentile for weight. Her temperature is 37°C (98.6°F), pulse is 90/min, respirations are 16/min, and blood pressure is 120/78 mm Hg. Examination shows conjunctival pallor and inflammation of the corners of the mouth. There are several tense, grouped subepidermal blisters on the shoulders bilaterally. The abdomen is soft, and there is diffuse tenderness to palpation with no guarding or rebound. Further evaluation of this patient is most likely to show which of the following findings?
A 32-year-old man with Crohn disease is brought to the emergency department after he fainted at work. He says that he has been feeling increasingly fatigued and weak over the last several weeks though he has not previously had any episodes of syncope. On presentation he is found to be pale and agitated. A panel of lab tests is performed showing the following: Hemoglobin: 10.2 g/dL Hematocrit: 30.1% Leukocyte count: 9,900 cells/mm^3 with normal differential Platelet count: 290,000/mm^3 Mean corpuscular volume: 118 µm^3 Elevated homocysteine level Normal methylmalonic acid level Which of the following mechanisms explains how Crohn disease may have contributed to this patient's symptoms?
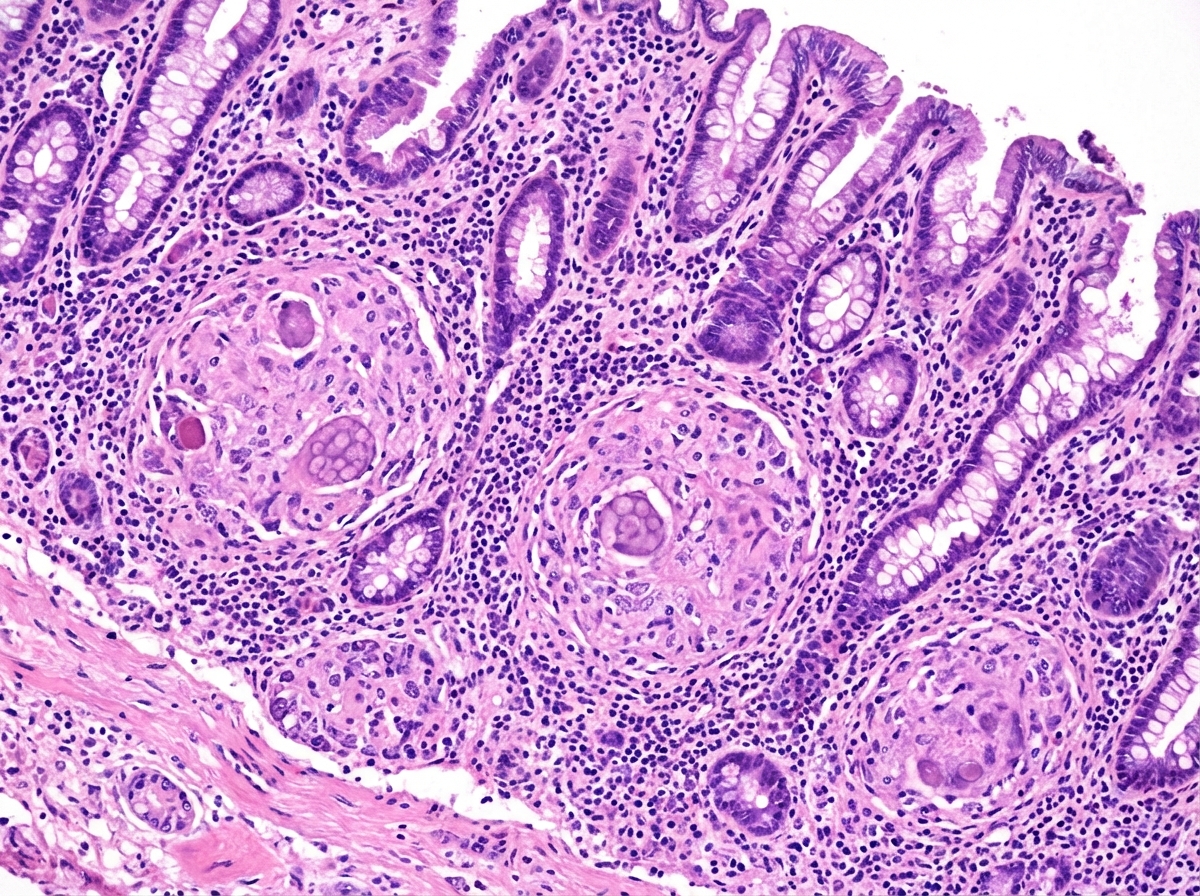
A 63-year-old man comes to the physician with a 4-week history of fatigue, crampy abdominal pain, watery diarrhea, and pain in his mouth and gums. He returned from a 2-week trip to the Dominican Republic 2 months ago. He has smoked one pack of cigarettes daily for 45 years. Examination shows three 1.5-cm, painful ulcers in the mouth. Abdominal examination shows mild tenderness to palpation in the right lower quadrant without guarding or rebound. His hemoglobin concentration is 11.2 g/dL, mean corpuscular volume is 75 fL, and leukocyte count is 11,900/mm³. Colonoscopy shows a cobblestone mucosa. A photomicrograph of a biopsy specimen is shown. Which of the following is the most likely diagnosis?
A 33-year-old man has a history of intermittent bloody diarrhea, tenesmus, fever, fatigue, and lower abdominal cramps for the past 2 weeks. On physical examination, he is lethargic and appears lean and pale. He has aphthous stomatitis, red congested conjunctiva, and tender swollen joints. At the doctor’s office, his pulse is 114/min, blood pressure is 102/76 mm Hg, respirations are 20/min, and his temperature is 39.4°C (102.9°F). There is vague lower abdominal tenderness and frank blood on rectal examination. Laboratory studies show: Hemoglobin 7.6 g/dL Hematocrit 33% Total leucocyte count 22,000/mm3 Stool assay for C.difficile is negative Abdominal X-ray shows no significant abnormality He is symptomatically managed and referred to a gastroenterologist, who suggests a colonoscopy and contrast (barium) study for the diagnosis. Which of the following is the most likely combination of findings in his colonoscopy and barium study?
A 31-year-old woman comes to the emergency department because of a 4-day history of fever and diarrhea. She has abdominal cramps and frequent bowel movements of small quantities of stool with blood and mucus. She has had multiple similar episodes over the past 8 months. Her temperature is 38.1°C (100.6°F), pulse is 75/min, and blood pressure is 130/80 mm Hg. Bowel sounds are normal. The abdomen is soft. There is tenderness to palpation in the left lower quadrant with guarding and no rebound. She receives appropriate treatment and recovers. Two weeks later, colonoscopy shows polypoid growths flanked by linear ulcers. A colonic biopsy specimen shows mucosal edema with distorted crypts and inflammatory cells in the lamina propria. Which of the following is the most appropriate recommendation for this patient?
Practice by Chapter
Crohn's disease pathophysiology
Practice Questions
Ulcerative colitis pathophysiology
Practice Questions
Diagnostic approach to IBD
Practice Questions
Extraintestinal manifestations
Practice Questions
Medical management of Crohn's disease
Practice Questions
Medical management of ulcerative colitis
Practice Questions
Biologic therapies for IBD
Practice Questions
Surgical management in IBD
Practice Questions
Nutritional considerations in IBD
Practice Questions
IBD in pregnancy
Practice Questions
Cancer risk and surveillance in IBD
Practice Questions
IBD-related complications
Practice Questions
IBD in special populations
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app